
Abstract
Abstract
Introduction
The institution of multimodal approaches (simultaneous use of ≥2 techniques with unique mechanisms of action or locations of action) to postoperative pain relief has been studied in general, orthopedic, thoracic, obstetric, and gynecologic surgical patients with varying results.3–8 The use of continuous wound infusion with local anesthetics has been incorporated into postoperative pain management plans as a proposed way to improve analgesia while decreasing narcotic use.
Continuous infusion of bupivacaine into surgical wounds of gynecologic oncology patients via use of the ON-Q PainBuster System® (I-Flow Corporation, Lake Forest, CA) is being applied today as part of a multimodal approach to postoperative pain management. Although the safety of this technique has been established, its efficacy has yet to be proven. There has only been one randomized controlled trial that studied use of continuous wound infusion in gynecologic oncologic patients. 9 The results of that study proved that the placement of wound-infusion catheters in the deep subcutaneous space was safe in this patient population, yet did not decrease pain scores or narcotic use. Another purely observational study described outcomes after intrafascial placement of infusion catheters. 10 Those researchers were able to reaffirm device safety; but, in contrast, concluded that the technique appeared efficacious for analgesia. To date, no studies have examined the efficacy of placement of soaker catheters below the fascia in this patient population. The objective of the current study was to determine if preperitoneal placement of continuously infusing bupivacaine catheters via the ON-Q PainBuster System resulted in decreased postoperative narcotic use in gynecologic oncology patients.
Materials and Methods
Institutional review board approval was obtained to perform this study. A retrospective chart review was conducted of all women who underwent open abdominal surgery for gynecologic malignancy at Thomas Jefferson University Hospital, Philadelphia, PA, between January 2007 and January 2011. Only patients who were admitted specifically for gynecologic surgery were included. Exclusions were: patients who were admitted for medical management prior to surgery, patients who were maintained on daily opiates for chronic pain disorders, patients undergoing concurrent nongynecologic abdominopelvic surgery, patients who died during the postoperative course, and patients with incomplete medical records. Data for each patient were abstracted from inpatient medical records (including operative reports, anesthesia records, and nursing notes).
Patients were divided into 2 groups: (1) women who did not have the ON-Q PainBuster system placed at the time of surgery (control group) and (2) women who did have the ON-Q PainBuster system placed at the time of surgery (study group). All soaker catheters were placed in a subfascial/preperitoneal location after the intra-abdominal portion of the procedure was completed and prior to fascial closure. Catheters were connected to pumps that were filled with 270 cc or 400 cc of either 0.25% bupivacaine or 0.5% bupivacaine, depending on surgeon preference. All catheters were removed between 72 and 96 hours after surgery, after the local anesthetic reservoir was found to be empty. All patients also received patient-controlled analgesia (PCA) pumps until they were able to tolerate oral (PO) intake, per routine care at this hospital. PCA pumps dispensed morphine, hydromorphone, or fentanyl, depending on surgeon and anesthesiologist preference. Eligible patients also received renally dosed intravenous (IV) ketorolac beginning on postoperative day #1, up to a maximum of 8 doses. Patients were transitioned to oral narcotic medications prior to discharge. Ibuprofen was also administered to patients on an as-needed basis to assist with pain control.
Demographic characteristics, medical/surgical history, tobacco use, alcohol use, tumor site/stage, and hospital stay were compared for both groups. Intraoperative characteristics (estimated blood loss, surgery time, and incision type) were also compared. The primary outcome was the total use of narcotics during the entire postoperative course. This outcome was divided into 3 subcategories: total narcotic use, IV narcotic use, and oral narcotic use. All narcotic doses were converted to IV morphine equivalents, using the guidelines made available through the Thomas Jefferson University Clinical Pharmacy prior to statistical analysis. Several secondary outcomes were also recorded, including maximum and minimum reported pain scores from postoperative day #0 through 5, total doses of antiemetics used, incidence of small-bowel obstruction or ileus (as diagnosed clinically and/or radiographically), fever (as defined as temperature ≥100.4°F), wound toxicity, need for transfusion, development of postoperative pneumonia, and diagnosis of deep-vein thrombosis or pulmonary embolism (DVT/PE).
All statistical analyses were performed using SPSS 17.0 (SPSS Inc., Chicago, IL). To summarize the data, frequency counts with percentages were tabulated for categorical variables and means with standard deviations were calculated for continuous variables. Fisher's exact tests and χ2 tests were used to analyze categorical variables. t-Tests were used to analyze continuous variables. A p-value of <0.05 was considered statistically significant.
Results
During the study period, a total of 200 patients who met inclusion criteria for this study were identified. Of these 200 women, 109 (54.5%) did not received intraoperative placement of the ON-Q PainBuster (control group) and 91(45.5%) did undergo intraoperative placement of the ON-Q PainBuster (study group). Table 1 presents comparisons of baseline demographics, social history, presence of medical comorbidities, prior surgical history, tumor site and stage, and length of hospital stay for both groups. No statistically significant differences were observed between the 2 groups. Intraoperative characteristics also did not differ significantly between the study and control group populations (Table 2).
Bold type indicates statistical significance.
BMI, body mass index.
Min, minutes; EBL, estimated blood loss.
The primary outcome of this study, postoperative narcotic use, was found to be significantly higher in the control group than the in study group (Table 3; Fig. 1). Patients in the control group consumed higher total doses of narcotics than did the patients in the study group (134.8 mg versus 92.8 mg, respectively; p=0.008), higher doses of IV narcotics (158.4 mg versus 100.9 mg, respectively; p=0.024), and higher doses of oral narcotics (23.9 mg versus 8.1 mg, respectively; p<0.001). Use of ketorolac and ibuprofen did not differ between the groups.
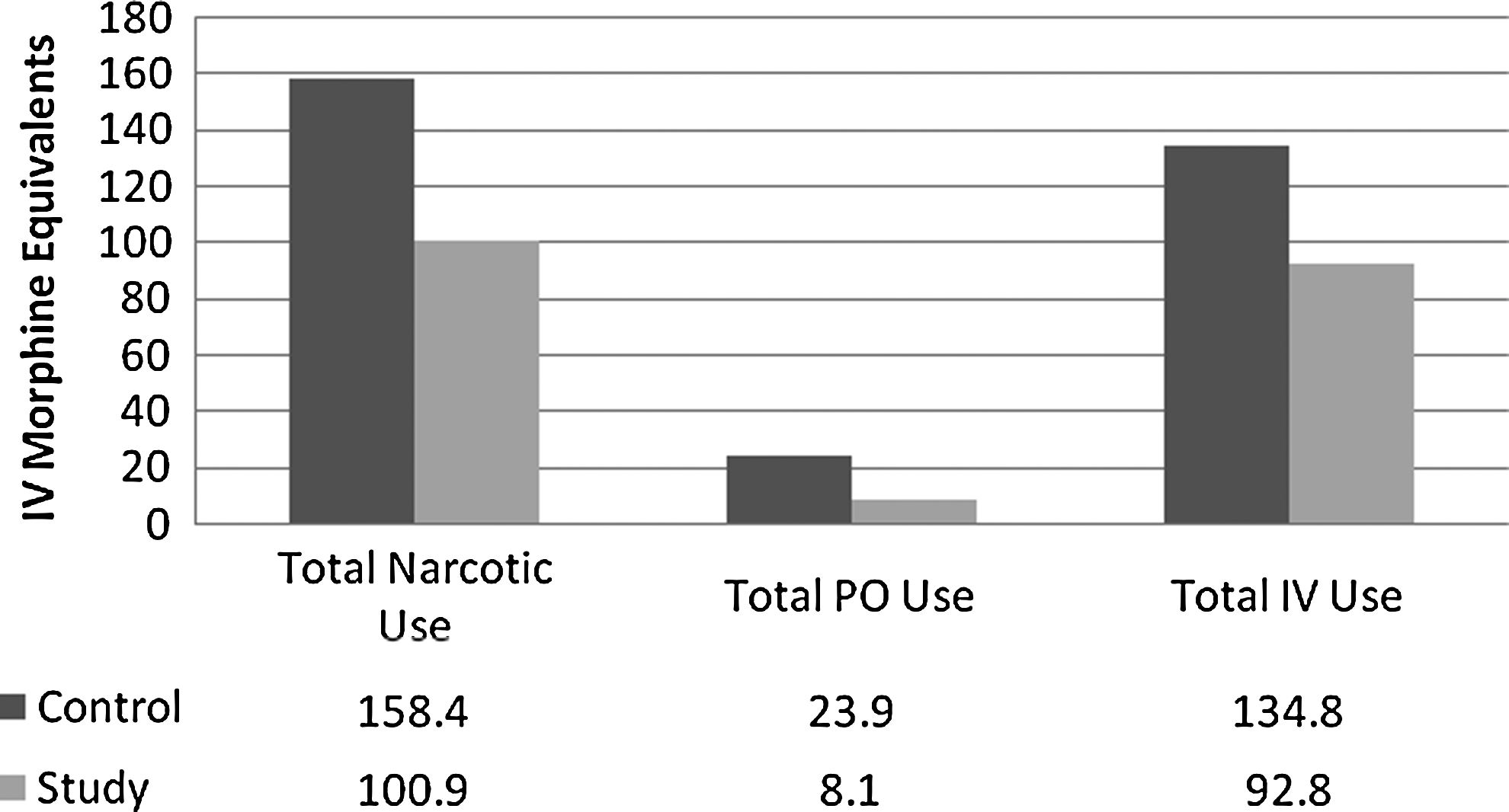
Postoperative narcotic use. IV, intravenous; PO, oral.
Bold type indicates statistical significance.
IV, intravenous; PO, oral.
Secondary outcomes are presented in Table 4 and Figure 2. No statistically significant differences were observed in both groups with regard to incidence of transfusion, wound toxicity, DVT/PE, or pneumonia. Patients in the study group required significantly fewer doses of antiemetics (0.8 versus 2.3, respectively; p<0.001) and also had significantly fewer diagnoses of small-bowel obstruction and ileus (4.4% versus 12.8%, respectively; p=0.038). Pain-score data were available for a total of 199 patients on postoperative days 0 and 1, 198 patients on postoperative day 2, 195 patients on postoperative day 3, 138 patients on postoperative day 4, and 75 patients on postoperative day 5. The maximum mean pain scores were significantly lower for patients in the study group than in the control group on postoperative days 2, 3, 4, and 5. On postoperative day 1, the mean maximum pain scores did not differ significantly between the 2 groups. Average minimum pain scores were significantly lower for patients in the study group than in the control group for all postoperative days. No complications with function of the ON-Q PainBuster pumps occurred, and all pumps were discontinued in the hospital prior to patient discharge.

Postoperative pain scores.
Bold type indicates statistical significance.
DVT/PE, deep-vein thrombosis/pulmonary embolism.
Discussion
Multimodal, analgesic, postoperative pain management has proven effective for surgical patients across many specialties. Specifically, the literature supports the use of local anesthetic wound infiltration as a component in these protocols. Studies that have examined its efficacy in gynecologic oncology patients, however, have yielded conflicting results. The current study sought to compare postoperative narcotic use retrospectively among patients treated with and without the preperitoneal ON-Q PainBuster system following gynecologic oncology surgery. It was found that the use of continuous wound infusion with bupivacaine resulted in significantly decreased narcotic use and reduced pain scores, without increasing wound toxicity.
A PubMed and Ovid search of the English-language literature identified no retrospective cohort studies investigating pre-peritoneal placement of continuously infusing bupivacaine catheters in a gynecologic oncology population. A randomized placebo-controlled trial by Kushner, et al. investigating the subcutaneous placement of infusion catheters failed to identify a significant difference in narcotic use or postoperative pain scores between patients randomized to wound infiltration with bupivacaine versus normal saline. 9 The current study differed not only in the location of catheter placement, but also in the exclusion of patients who did not have a cancer diagnosis. A second study by Shen-Gunther examined placement of infusion catheters within the rectus sheath. Although these researchers were able to demonstrate that use of the ON-Q system was efficacious and safe, that study included patients with benign disease, lacked a control population, and was purely observational. 10
Shen-Gunther's description of somatic neuroanatomy and peripheral nociception provided an anatomical and neurologic rationale for the success of preperitoneal local anesthetic infusion. 10 The rectus abdominis muscle is innervated by the lower 6 intercostal nerves for which terminal branches travel posteriorly to the internal oblique muscles. Incisional pain after laparotomy has been attributed to the incision and subsequent closure of the fascia and linea alba under tension. Placing catheters in the preperitoneal space, where infiltration of the fascia and rectus muscles is possible, provides an anatomic basis for Shen-Gunther's, 10 Kushner et al.'s 9 and the current study's results.
Postoperative nausea, emesis, and ileus are a few of the most common causes of an extended hospital stay in surgical patients. 11 The current study group subjects required fewer antiemetics and had fewer diagnoses of ileus and obstruction. The current authors attributed this to decreased use of systemic opiates, the side-effects of which include nausea, vomiting, and delay of bowel function, and to the effects of local anesthetics in promoting postoperative bowel motility through reduction of inflammation and potentiation of intestinal smooth-muscle contraction.2,12,13 Although patients with ON-Q Pain Buster catheters were diagnosed with fewer cases of ileus and small-bowel obstruction, this did not translate into a reduction in hospital stay. This finding may also be attributed to factors that were not studied directly, including social support, medical comorbidities, patient preferences, surgeon expectations, and discharge planning. A post-hoc power analysis was conducted. The power of this study was 0.33 (α=0.050, 2-tailed) to detect a difference in length of hospital stay which was probably reflective this study's small sample size.
A limited cost analysis of patients in this study demonstrated that use of the ON-Q PainBuster system was not cost-effective in gynecologic oncology patients. In the authors' institution, the cost for a 50-cc syringe of morphine used in a PCA infusion pump is approximately $82, wheras the cost for a 270-cc ON-Q PainBuster system is approximately $315 ($200 for the device and $115 for local anesthetic), and the cost for a 400-cc ON-Q PainBuster system is approximately $414 ($300 for the device and $115 for local anesthetic). Thirty-four patients in the study group had 270-cc ON-Q PainBuster pumps placed, while the remaining 57 patients had 400-cc ON-Q PainBuster pumps placed. Given that patients in the study group required a mean of 92.8 morphine equivalents for pain control in addition to receiving local anesthetic through the ON-Q PainBuster devices, the approximate cost of this pain-control regimen would be $466 for patients who received a 270-cc pump and $566 for those who received the 400-cc pump. Patients in the control group required a mean of 134.8 morphine equivalents throughout their stays. The approximate cost for this pain-control regimen would be approximately $221 per patient. From a purely cost-based perspective, the use of the ON-Q PainBuster pump in this patient population cannot be recommended.
Limitations of this investigation included a small sample size, location within a tertiary-care facility, and the retrospective nature of the study design. Because patients in the study group were not blinded, patient expectations of improved pain control with the use of the ON-Q PainBuster system may have influenced their fewer requests for narcotics. In addition, drawing the study population from a single tertiary-care institution limited its external validity.
Conclusions
The results of this demonstrate that pain control is improved without increased frequency of complications with the use of local anesthetic wound infiltration. This study sets the groundwork for conducting a randomized, placebo-controlled double-blinded trial using preperitoneal placement of the ON-Q PainBuster system in gynecologic oncology patients.
Footnotes
Disclosure Statement
No competing financial conflicts exist.