
Abstract
Abstract
Introduction
Case
A 15-year-old girl with lower abdominal pain on her third menstruation day consulted her doctor, who prescribed antibiotics for suspected gastroenteritis. This patient had had her menarche when she was 13 years' old and was still a virgin. She usually took psychotropic drugs (etizolam and fluvoxamine maleate) for a maladaptative psychiatric condition and was receiving psychiatric counseling.
After 3 days, her temperature rose to 38°C, and she felt more-severe right lower abdominal pain. She went to a hospital near her home, where she was admitted. She received antibiotic treatment for 6 days, but her pain remained, though she no longer had a fever. She underwent abdominal ultrasonography and computed tomography (CT), which revealed a cystic mass proximal to the uterus. Because torsion of an ovarian cyst was suspected, she was referred to the current authors' hospital for further evaluation and treatment on the seventh day after admission.
When this patient arrived at the new hospital, her abdomen was generally soft and flat except for mild tenderness and rebound tenderness in the right lower quadrant of the abdomen. Her height and weight were 164 cm and 67 kg, respectively, and she had a temperature of 36.9°C. Her blood pressure was 125/80 mm Hg with a pulse rate of 115 beats per minute. Her laboratory data, including a complete blood count were as follows: white blood cells, 5800/μL; red blood cells, 3.73×106/μL; hemoglobin, 9.1 g/dL; hematocrit, 29.8%; platelets, 35.1×104/μL; aspartate aminotransferase, 13 international units (IU)/L; alanine aminotransferase, 11 IU/L; lactate dehydrogenase, 23 IU/L; blood–urea–nitrogen, 5 mg/dL; creatinine 0.5 mg/dL; total bilirubin, 0.2 mg/dL; C-reactive protein, 1.60 mg/dL; cancer antigen (CA) 125, 83.4 U/mL; CA 19-9, 5.1 U/mL; α-fetoprotein, <1.0 ng/mL; and Chlamydia antibodies, immunoglobulin (Ig)A (–), IgG (–).
Transabdominal ultrasonography showed a normal uterus and a cystic structure measuring 85×66 mm in the left side of the uterus (Fig. 1). On magnetic resonance imaging (MRI), the cystic tumor was noted to contain blood that was hyperintense on T1-weighted imaging (Fig. 2A) and hypointense on T2-weighted imaging (Fig. 2B).
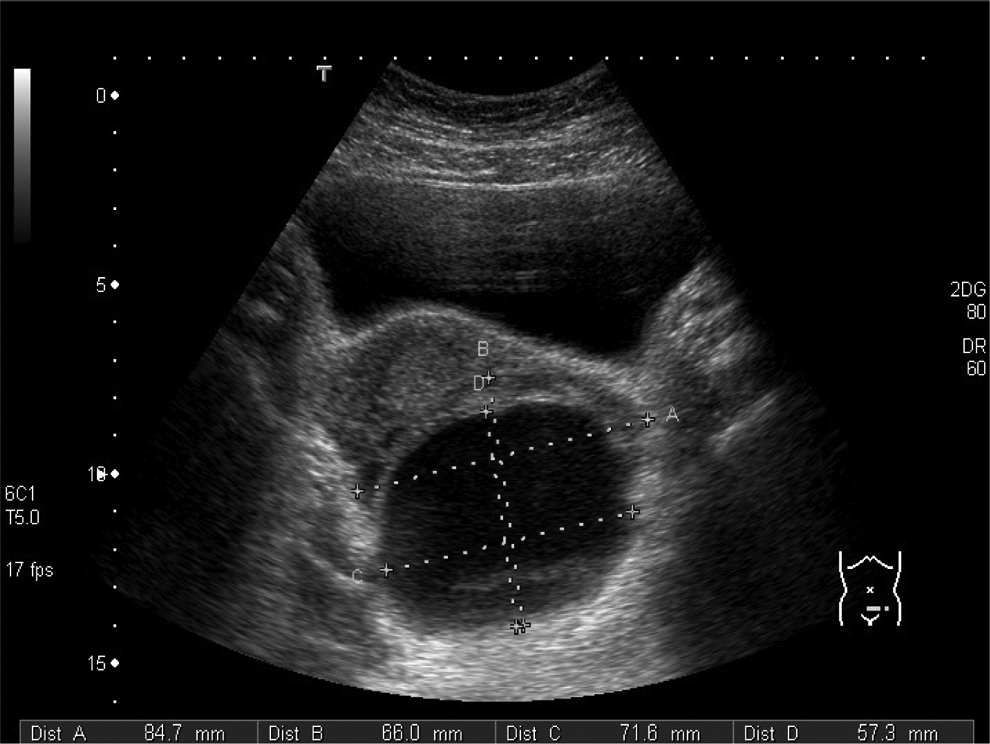
Ultrasonography. Abdominal sonography shows a cystic mass that contains a solid tumor, measuring 85×66 mm in the left side of the uterus.

Magnetic resonance imaging (MRI). Axial T1-weighted MRI
Because she continued to experience pain, it was decided to perform an urgent laparoscopy according to the indication for the diagnosis of torsion of the left tumorous ovary. Laparoscopy revealed torsion of the right fallopian tube with necrosis and swelling. The fallopian tube was twisted three complete turns clockwise (Fig 3A).
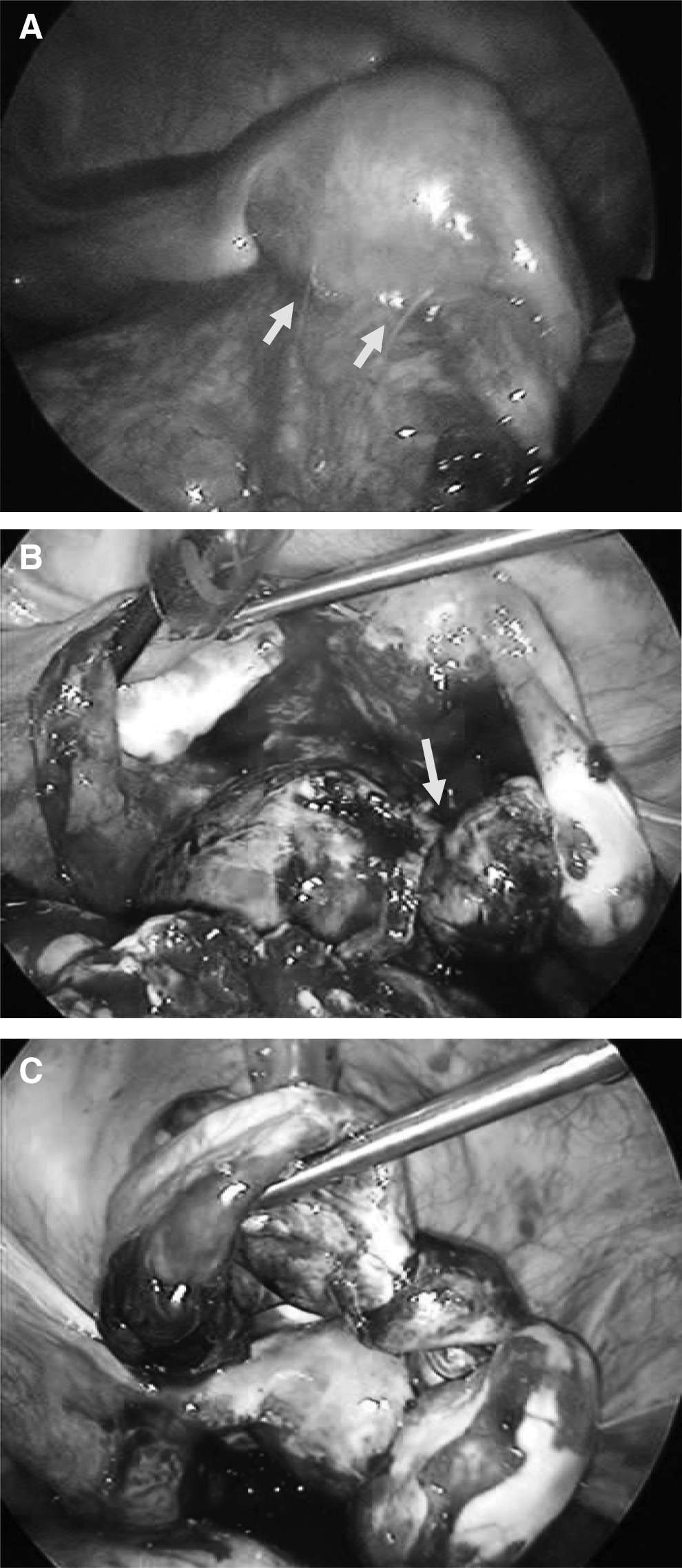
Findings during laparoscopy.
The uterus, bilateral ovaries, and left fallopian tube were normal. Adhesion of the greater omentum was prominent around the uterus and both adnexa (Fig. 3B). The cyst was punctured, using a double balloon catheter (Hakko Medical Inc., Tokyo, Japan), and the cyst contained 120 mL of hemorrhagic liquid (Fig 3C). As it was difficult to preserve the fallopian tube, laparoscopic right salpingectomy was performed. The excised right tube looked like a cyst with edematous and necrotic changes of ampulla of the fallopian tube (Fig 4). Pathologic examination revealed marked necrosis and hemorrhagic changes without any evidence of malignancy.

Specimen. The right isthmus of the fallopian tube is extended like a cyst. Edematous and necrotic changes were seen in the ampulla of the fallopian tube.
Results
The patient was discharged uneventfully on the third day after surgery.
Discussion
While the common cause of gynecologic acute abdomen may be ovarian tumor torsion mostly of the fallopian tube, isolated torsion of the fallopian tube is very rare, as the reported incidence is 1 in 1,500,000 women. 1 Gynecologists usually encounter this condition in women of reproductive age but rarely in adolescent and menopausal women.
Expected factors for torsion of the fallopian tube are anatomical abnormalities (congenital abnormalities of the mesosalpinx or fallopian tube, hydrosalpinx, hematosalpinx, and ovarian or paraovarian tumors), local physiologic abnormalities (hypermotion of the tube or spasm of the tube caused by drugs), hemodynamic abnormalities (venous congestion in mesosalpinx), trauma, sudden body movement, previous operation (such as tubal ligation), previous disease (pelvic inflammatory disease [PID]), and pregnancy.2,3
In another study by Tirso et al., fallopian-tube torsion was caused by genital tuberculosis in woman with no history of sexual intercourse. 4 In most cases, it is difficult to discover a definite cause for fallopian-tube torsion. Milki and Jacobson. reported that torsion of the right fallopian tube is more commonly described than that of the left fallopian tube. 5 It could be that mobility of the left fallopian tube is limited by the sigmoid colon or that there is slow venous flow on the left side, which results in congestion. 5
When patients present with symptoms of abdominal pain, nausea, and vomiting, differential diagnosis includes torsion and rupture of the ovary, appendicitis, PID (such as an adnexitis), urinary-tube infection, and urinary calculus.
In adolescence, the common course of acute lower abdominal pain is appendicitis. Because fallopian-tube torsion has no pathognomonic, specific symptoms nor any laboratory data, it is difficult to diagnose preoperatively.
Sonography, CT, and MRI are useful for diagnoses of this disease. Sonography is convenient and could provide useful information about ovarian blood flow via color Doppler imaging to estimate the viability of the target organ. CT and MRI findings of fallopian-tube torsion include a normal ipsilateral ovary, thickness of the tubal wall, an adnexal cyst with a dilated fallopian tube, deviation of uterus to the torsional side, and a “beak sign”—a term that is applied when the mass that deforms the edge of an adjacent organ has a beaklike shape, suggesting that the mass arises from the organ. 6
Park et al. reported that CT and MRI scanning depict the coiling-up sign of the torsioned fallopian tube, which is helpful for diagnosing isolated tubal torsion. 7 In the present case, the appearance of the coiling-up sign was shown next to a cystic lesion (Figs. 5 A and B).

A coiling-up sign on magnetic resonance imaging (MRI).
Torsion of the hematosalpinx was detected via laparoscopy. The hematosalpinx might have caused the tubal torsion or could have been a result of that torsion. Therefore, it is difficult to determine definitively which was the initial event. However, in addition to the definite identification of the hematosalpinx, or the torsion as an initial event, it could be speculated that both events create a vicious cycle.
Twenty-four case reports of fallopian-tube torsion in teenagers were published in the 29 years from 1981 to 2009 (Table 1).8–30 There were 8 premenarchal and 9 unknown cases. Most likely, all cases were of girls with no history of sexual intercourse. In most cases, preoperative ultrasonography was carried out, when 3 cases were preoperatively diagnosed correctly as fallopian-tube torsion. Other preoperative diagnoses were torsion of an ovarian cyst (n=4), appendicitis (n=3), torsion of a paraovarian cyst (n=2), a cystic ovarian follicle with ovulatory pain (n=1), and an adnexal tumor (n=1). In other cases there was no diagnosis (n=10).
Ex of inter, experience of intercourse; Preoperative dx, preoperative diagnosis; Time interval, time interaval between onset of pain to surgery; LAP, lower abdominal pain; Vo, vomiting; S, sonography; C, computed tomography; M, magnetic resonance imaging; X-ray, abdominal X-ray; Lt, left; Rt, right; Rec, recurrence; Lap, laparascopic; Abd, abdominal; n/d, not described.
Laparoscopy was performed in 19 cases, and laparotomy was chosen in 4 cases. There was 1 case for which the treatment procedure was not described. In the last 5 years, laparoscopy was performed in all of cases from that point onward. Therefore, it should be noted that laparoscopy currently plays an important role in diagnosis and treatment.
The surgical technique for addressing this disease is release or resection of the torsional salpinx. The current authors usually tend to determine the necessity for salpingectomy intraoperatively when gross inspection of the twisted fallopian tube is possible. However, in fact, there is no established rule for resection of the affected tube at present.
In the literature that was reviewed, 19 cases were treated by salpingectomy, 1 case by adnexectomy, and 3 cases by detorsion. Because this disease usually occurs during the reproductive period of the lifecyle, preserving fertility is important. Therefore, further consideration is warranted to establish a standard for preserving the fallopian tube. As time passes from the onset of this condition, blood circulation became worse because of the torsion. As a result, the range of necrosis will spread. In literatured reviewed, the range of time between the onset of pain to the operation was 1 day to 1 year. For preserving fertility, it is necessary to have prompt diagnosis and surgical intervention. Especially in adolescence, as in the present case, the diagnosis of this disease is often likely to be delayed. Because there are no characteristic symptoms, patients often have to undergo prolonged investigations to rule out the more common causes of the abdominal pain. In adolescence, patients first usually consult a pediatrician and then, if deemed necessary, they consult a gynecologist. It is necessary, therefore, to be in close communication with other physicians to enable prompt diagnosis and treatment. Laparoscopic treatment is less invasive and especially useful for diagnosis and treatment in these cases.
Conclusions
The current authors reported torsion of the fallopian tube in adolescence. It was difficult to make a preoperative diagnosis in this disease. Laparoscopy was effective for diagnosis and treatment. Park et al. have described a coiling-up sign that shows on MRI imaging that is a specific sign of fallopian-tube torsion. 7 In the current case, this sign was discovered retrospectively on the MRI. This sign aids in making preoperative diagnoses. In cases of fallopian-tube torsion, prompt diagnosis and treatment is required to preserve fertility. Although fallopian-tube torsion is a rare disease in adolescent girls, it should be considered as part of the differential diagnosis of acute lower abdominal pain.
Footnotes
Acknowledgments
The authors would like to express great gratitude to Eiko Yamashita, MD, in the department of radiology, at the Tokai University School of Medicine, for her helpful comments on MRI.
Disclosure Statement
No author has any conflict of interest in connection with this article.