
Abstract
Abstract
Introduction
Case
A 26-year-old woman (gravida 0) presented to the emergency department with a 1 day history of left lower quadrant abdominal pain. The pain was sudden in onset, had begun when the patient was swimming the previous day, and subsequently grew worse. Although her pain was not associated with fever, chills, nausea, vomiting, diarrhea, vaginal bleeding, or dysuria, she reported subjective fullness in her abdomen. Her last menstrual period had been 3 weeks previously, and her gynecologic, medical, and surgical history was unremarkable. Vital signs were within normal limits, but abdominal examination revealed left lower quadrant tenderness associated with involuntary guarding and rebound tenderness. Pelvic examination was significant for a 20 week sized uterus associated with tenderness, with no adnexal tenderness or enlargement. The patient's urine pregnancy test was negative and the initial hemoglobin level was 12.3 g/dL.
Transabdominal and transvaginal sonography of the pelvis showed a 22×12×14 cm heterogeneous mass in the midline of the pelvis superior to the uterine fundus and containing color flow. The uterus and ovaries were well visualized and looked normal. A computed tomography scan of the abdomen and pelvis was performed to further visualize the mass, and the mass was noted to be circumscribed and heterogeneous, originating from the pelvis. Free fluid was noted in the inferior perihepatic region, left paracolic gutter, and pelvis. No lymphadenopathy or peritoneal abnormality was noted. Given these findings and the presence of acute abdominal signs, an exploratory laparotomy was performed. Upon peritoneal entry, 1000 mL of hemiperitoneum was noted. Blood admixed with clots was found in the left paracolic gutter as well as the anterior and posterior cul-de-sacs. A large pedunculated pelvic mass with solid and cystic components was found attached to the posterior wall of the uterine fundus by a thick stalk (Fig. 1). Although the stalk was intact, bleeding was noted from an avulsed adhesion between the left broad ligament and the pelvic mass. The stalk was clamped and the mass was excised (Fig. 2). Hemostasis was achieved with simple hemostatic stitches.

Intraoperative view of the mass attached to the posterior wall of the uterine fundus.

Excised surgical specimen.
On gross inspection, the mass was intact, bilobed, and encapsulated with a pink-tan, glistening, and smooth surface. The mass weighed 2130 g and measured 24×17×7.5 cm. In the center of the bilobed mass was an attached portion of tan-pink to red, partially cauterized tissue measuring 2.8×2.2×0.5 cm, representing the attachment point to the uterus. The mass was serially sectioned along the long axis and revealed a white-tan to pink, homogeneous cut surface having a myxoid fibrous appearance with surrounding copious edematous tissue. Three foci of hemorrhage ranging from 1 to 4 cm in greatest dimension were identified.
Detailed histologic evaluation of the excised mass showed a smooth muscle neoplasm with multifocal areas of nuclear atypia (Fig. 3). A mitotic count was performed within multifocal areas, which revealed one mitosis within 50 high power fields. No areas of coagulative necrosis or vascular invasion were identified. Immunohistochemical analysis was positive for alpha smooth muscle actin and desmin but negative for S100, CD31, and CD34. These findings were consistent with a symplastic leiomyoma. Additionally, intraparenchymal hemorrhage was present within the leiomyoma. The area of attachment was examined histogically, revealing negative margins. Therefore, the leiomyoma was thought to be completely excised. The patient was discharged on postoperative day 2 with a hemoglobin level of 9.8 g/dL. Postoperative recovery was unremarkable.
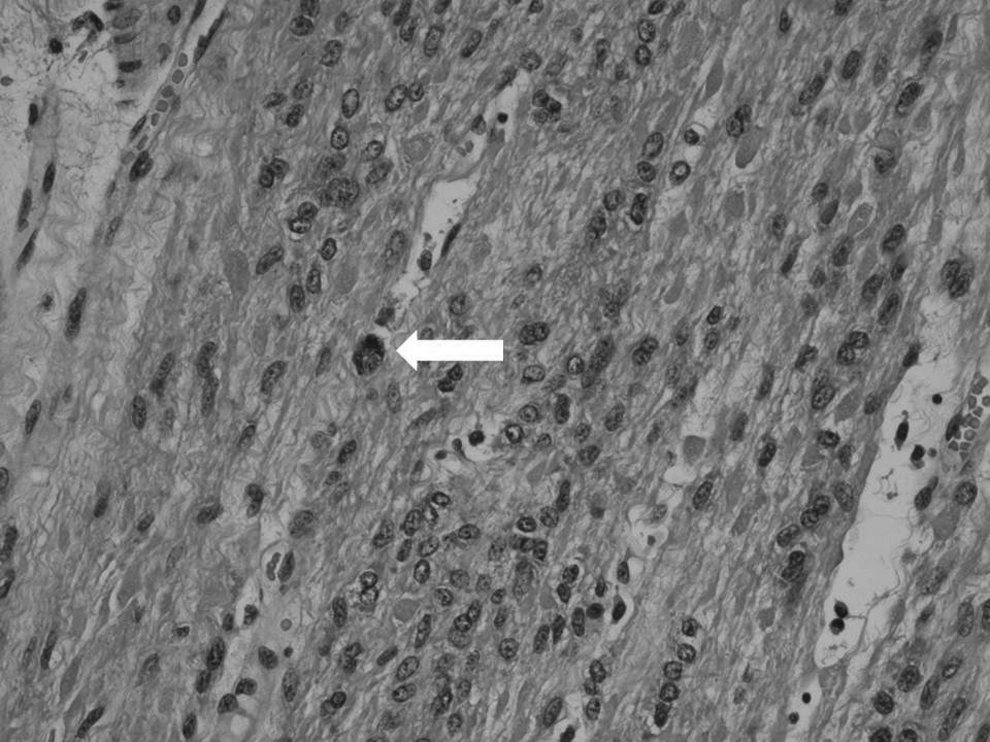
Photomicrograph of excised tumor (200×) shows mitosis (arrow).
Discussion
Acute abdominal pain in a woman of reproductive age can be caused by a multitude of factors, which can prove to be a diagnostic challenge. Apart from meticulous clinical history, physical examination, and pregnancy testing, radiologic imaging is important in the evaluation of any woman with abdominal pain. In this case, left lower quadrant abdominal tenderness with a negative pregnancy test and tender 20 week sized uterus raised the suspicion of pelvic pathology. In the initial differential diagnosis, gynecologic causes were considered, including ovarian or adnexal torsion, rupture of a corpus luteum cyst, rupture of a peritoneal or pelvic abscess, or torsion or rupture of a pelvic tumor of uncertain malignant potential. Also considered were other nongynecologic causes such as perforated bowel, sigmoid volvulus, and diverticulitis. Based on initial ultrasonography adnexal pathology was ruled out; however, the presence of a large pelvic mass warranted further radiologic evaluation to delineate the source and extent of the mass. Given computed tomography findings of a large pelvic mass, the absence of other gastrointestinal findings, and the presence of acute abdominal signs, an exploratory laparotomy was indicated. Prior to surgery, torsion or rupture of a pelvic tumor of uncertain malignant potential was high in the differential diagnosis. Intraoperative findings further reinforced the diagnosis of a pedunculated uterine tumor.
The degree of hemoperitoneum upon peritoneal entry was interesting, and it is hypothesized that the hemoperitoneum was the cause of the patient's peritoneal signs. Massive hemoperitoneum has been known to result from rupture of aberrant vasculature associated with uterine leiomyomas.9–13 Inciting factors in these cases range from minimal activity to defecation and exercise. In one case, a patient developed life-threatening hemoperitoneum resulting from post-traumatic avulsion of a pedunculated uterine leiomyoma (fall while jogging). 14 Similarly, patient's hemoperitoneum possibly resulted from the avulsion of an adhesion between the symplastic leiomyoma and the left broad ligament that may have occurred traumatically, that is, while she was swimming. This may explain why it took almost an entire day for hemoperitoneum to develop from the gradual bleeding arising from the serosa of the broad ligament. It is unlikely that the leiomyoma was hemorrhagic, as the tumor was well circumscribed and histologically inconsistent with hemorrhage. Theoretically, torsion of the pedunculated leiomyoma could also have caused hemoperitoneum, particularly if the uterine fundus was involved; however, the presence of a thick, intact stalk makes this less likely.
Although uterine smooth muscle tumors range from benign leiomyomas to malignant leiomyosarcomas, several intermediate histologic variants are associated with different types of cellular architecture, growth patterns, and malignant potential. 2 These variants are also associated with confusing nomenclature that although histologically accurate provides little clinical or prognostic information. 2 Symplastic leiomyomas are synonymous with atypical leiomyomas, pleiomorphic leiomyomas, and leiomyomas with bizarre nuclei. They are characterized by pleiomorphic nuclei and diffuse or multifocal moderate to severe atypia and low mitotic activity (<10 mitotic figures/10 high power fields) and show no evidence of tumor cell necrosis. 2 Leiomyosarcoma, conversely, usually exhibits diffuse moderate to severe atypia, a mitotic count of >10 mitotic figures/10 high power fields, and evidence of tumor cell necrosis. 2 These tumors are not limited to the uterus; atypical leiomyomas have been found in the bladder, scrotum, vagina, broad ligament, skin, nose, and even colon.6,15–21
Conclusions
Symplastic leiomyomas follow a benign clinical course and are considered by many experts to have little or no recurrence or metastatic potential.2,22 Although an association of uterine leiomyosarcomas with symplastic or atypical leiomyoma-like areas has been reported, long-term data reveal limited or no metastatic potential.5,22 This is further supported by a recent clinical study involving 13 patients treated with myomectomy for symplastic leiomyomas (followed between 20 and 151 months) in which no patient developed metastasis and only 1 developed local recurrence at the myomectomy site after 22 months. 23 On the basis of these findings, this patient was counseled that her prognosis was excellent. Although frequent screening for recurrence was not recommended nor were fertility problems foreseen, it was explained to her that recurrence was theoretically possible, and follow-up was recommended if she developed new symptoms.
Footnotes
Acknowledgments
We thank Jie Xu, Department of Obstetrics and Gynecology, Drexel University College of Medicine, for images and Diana Winters, Academic Publishing Services, Drexel University College of Medicine, for manuscript preparation.
Disclosure Statement
No competing financial conflicts exist.