
Abstract
Abstract
Introduction
Until 1970, >80% of ectopic pregnancies were recognized after rupture. With the excellent resolution afforded by transvaginal sonography (TVS), the high sensitivity of radioimmunoassay of β-human chorionic gonadotrophin (hCG), and the increased vigilance of clinicians, >80% of ectopic pregnancies now are detected before rupture.1,3
Therapeutic options for women with tubal ectopic pregnancy are surgery, medical treatment, or expectant management. In surgery, laparoscopy is now the accepted approach to performing salpingotomy or salpingectomy. Concerning medical treatment, systemic administration of methotrexate has gained acceptance in selected patients.4–6
Laparoscopic surgery has the following advantages: 1) relatively wide spectrum of indications; 2) easier operative conversion to laparotomy based on definite diagnosis under direct view; 3) evaluation of intraperitoneal findings other than the ectopic pregnancy; and 4) less invasiveness, which results in shorter hospital stay and faster return to everyday life, compared with laparotomy.4,7,8
A well-recognized hazard after salpingotomy is persistent trophoblast. The risk of persistent trophoblast tissue (PTT) after salpingotomy is reported to be 2%–11% with laparotomy and 5%–20% with laparoscopy.9–11 Prophylactic methotrexate results in fewer cases of tubal rupture (0.4% vs. 3.7%) than does surgery without methotrexate. 12 Known side effects of methotrexate include stomatitis, gastroenteritis, leukopenia, transaminitis, thrombocytopenia, and pneumonitis.6,9,10 Also, methotrexate-associated complications occur more frequently with prophylaxis (5.5% vs. 0.8%). 12 Attention should be paid to the possible occurrence of PTT, because if not detected at an early stage, it may result in intraperitoneal hemorrhage and shock, which necessitates emergency surgery to resect the fallopian tube.9–11 Consequently, it is important to monitor serum β-hCG levels until they become undetectable. Prophylactic methotrexate at the time of linear salpingostomy for the treatment of ectopic pregnancy is preferable to observation when a patient is at increased risk of PTT, such as in instances of small ectopic pregnancies (<2 cm), lesser gestational age, and rapidly rising preoperative hCG levels. 12
In the present study, an attempt was made to postpone the immediate postoperative prophylactic methotrexate for 2 or 4 days postoperatively, which would be given only to patients with suspected PTT and not to all laparoscopic salpingotomy patients with tubal ectopic pregnancy. Some patients can avoid the use of valueless methotrexate therapy.
Patients and Methods
This prospective pilot study was performed at the Department of Obstetrics and Gynecology of Alhammadi Specialized Hospital, Riyadh, Saudi Arabia. All women with laparoscopically confirmed diagnosis of tubal pregnancy who were candidates for linear salpingotomy were eligible for this study. All women gave informed consent before entering the operating room. Prior approval for the study had been obtained from the institutional review board.
All women had had discussions about methods of treatment for ectopic pregnancy. All women who elected to have medical treatment with methotrexate rather than a conservative surgical procedure were excluded from the analysis. Women who accepted linear salpingotomy were told about prophylactic methotrexate or waiting for follow-up with β-hCG results, to receive methotrexate only if there was an unsatisfactory decrease in β-hCG detected postoperatively. Women were informed about the importance of follow-up post-surgery to avoid the risks of PTT. Full patient addresses and contact telephone numbers were collected. Fortunately, all patients had regular follow-up.
The outcome measure was treatment success, defined as the complete elimination of trophoblast tissue with an uneventful decline of serum β-hCG to nonpregnant levels <5 milli-international units (mIU)/mL. Repeat interventions (medically by methotrexate or surgically by salpingectomy) for either clinical symptoms or inadequately declining serum hCG levels, that is, PTT, were therefore considered as treatment failures.
Ectopic pregnancies were diagnosed by evaluation of the patient's clinical history, gynecologic examination, TVS, and measurement of serum β-hCG levels. The criterion for ultrasound was the presence of an extraovarian adnexal mass in patients with a suspected ectopic pregnancy (amenorrhea, bleeding, and pain) who tested positive for β-hCG.
TVS was performed using a 7.5-MHz transvaginal probe with Synerg equipment (General Electric, Milwaukee, WI). Serum β-hCG concentrations were measured using an enzyme immunoassay kit (AIA-pack beta-hCG, Tosoh Medic, Inc., Yamaguchi, Japan).
Hemodynamically stable women with a presumptive diagnosis of tubal ectopic pregnancy, scheduled for surgery, were eligible for inclusion. The decision to perform linear salpingotomy was made by the surgeon on the basis of intraoperative findings. Candidates for linear salpingotomy included patients without tubal rupture and those who had an ectopic pregnancy in the ampulla or infundibulum of the fallopian tube, and desired to preserve fertility.
The laparoscopic procedure was performed according to that previously described by Pouly 13 and Tulandi and Saleh. 14 For the laparoscopic procedure, the patient was placed in a steep Trendelenburg position, legs apart, with the fixation of an intracervical adapter by vacuum to allow movement of the uterus and possible tubal chromopertubation. All procedures were performed with the patient under general anesthesia. The CO2 insufflation was performed up to an intraabdominal pressure of 14 mm Hg. In addition to the 10 mm umbilical incision, laparoscopic skin incisions, lateral to epigastric arteries, were performed bilaterally for the introduction of two operating trocars (one 10 mm and one 5 mm) that were inserted by means of lateral suprapubic incisions. In cases of hemoperitoneum, aspiration and washing of the pelvis was done with saline solution under pressure using the Hamou Endomat (Karl Storz Endoscopy‐Japan Inc.). For unruptured tubal (in the ampulla or infundibulum) pregnancies, the tube was identified and mobilized. A 10–20 mm incision for linear salpingotomy was made in the antimesenteric proximal portion of the hematosalpinx using a fine‐tip needle cautery or knife electrode (Karl Storz Endoscopy‐Japan Inc.). The irrigation and suction tube was introduced through the salpingotomy incision, and all clots and trophoblastic tissues were aspirated, after which saline solution was injected under high pressure with the Hamou Endomat, in an attempt to separate the trophoblast from the tubal wall. Depending upon the size, the products of conception were removed through a 5 or 10 mm trocar sleeve after grasping the tissue and passing through the operating channel of the laparoscope or the tissue was then placed in an endoscopic bag and removed from the abdominal cavity. After the tissue was removed, the tube was irrigated carefully and checked for hemostasis. The tube was then left to heal by secondary intention. The surgeon removed all clots and products of conception, and assessed the contralateral fallopian tube. Oozing from the tube is common but usually ceases spontaneously. Occasionally, coagulation is necessary. If any bleeding or oozing of blood from inside the lumen or tubal wall occurred that was not easily controlled, or the procedure was associated with complete tubal damage, such cases were switched to salpingectomy, but fortunately, that was not done in any cases in the current study.
During surgical procedure, the following concepts and techniques were considered:6,9,14–16
• The salpingotomy must be as nontraumatic as possible. The crucial point is to avoid large coagulation of the tubal wall, which can lead to a tuboperitoneal fistula. Therefore, it must be achieved with a fine electrode and a cutting current. The electrode must not be pressed on the tube, but rather should just touch it slightly to increase the power density. The speed of movement along the incision must be sufficiently fast to maximize the cutting effect and limit the collateral coagulation. Bipolar coagulation is forbidden for this step. • The salpingotomy must be performed at the internal part of the hematosalpinx. The trophoblast is located there, and the distal part contains generally only clots. Aspiration of the trophoblast must be performed with a suction device that is at least 7 mm in internal diameter. With a narrower device, the risk of partial removal of the trophoblast increases. The high rate of failure in some series is largely explained by the use of inefficient suction devices.
15
• The tube must be washed and explored to ensure complete removal of the trophoblast. It appears as a white tissue that can be removed using repeated suction or by grasping it gently with forceps. • The salpingotomy must not be sutured, as it has been proven that suturing the tube increases the risk for obstruction and decreases postoperative fertility, and that the tubal scar quality is better without a suture.
16
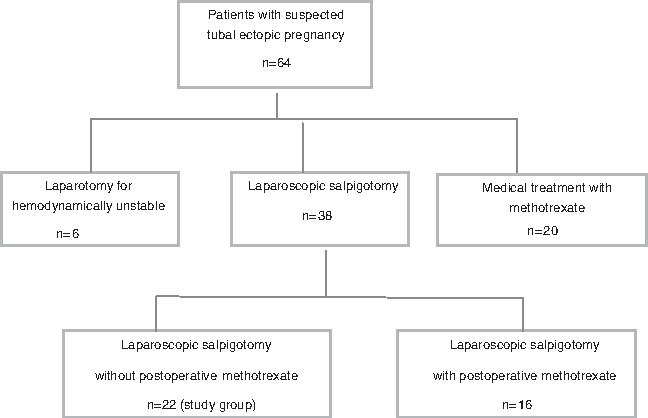
Flow chart of participants with tubal pregnancy.
If the serum β-hCG concentration declined by at least 50% and 75% at 2 and 4 days postoperatively, the measurement was repeated weekly until the concentration dropped to nonpregnant value. The immediate response to debulking the ectopic mass is a significant drop in β-hCG titers. It can take few weeks for residual trophoblast to grow and influence the titers. Titers need to be followed until reaching nonpregnant level.
The diagnosis of suspected PTT after laparoscopic salpingotomy is made by 2 days postoperatively; the β-hCG level should be <50% of the preoperative level, and, after 4 days, <25% of the preoperative level. 8
In the current study, methotrexate was indicated when PTT was suspected. Exclusion criteria for methotrexate were: hepatic (serum aminotransferase concentrations more than twofold the normal level), renal (serum creatinine concentration>1.5 mg/dL), or hematologic dysfunction (leucopenia<2000/mL, thrombocytopenia<100 000/mL); suprarenal gland dysfunction; active pulmonary disease; peptic ulcer disease; overt or biological evidence of immunodeficiency; or known sensitivity to methotrexate. The dose of intramuscular methotrexate was 50 mg/m2 body surface area. The day on which a woman received methotrexate was considered day 1. Serum β-hCG was measured again on days 4 and 7 after methotrexate injection. If the concentration did not decline by at least 15% between days 4 and 7, a second dose of methotrexate was administered. If the serum β-hCG declined by at least 15%, the measurement was repeated weekly until the concentration reached nonpregnant level. Failure of the serum β-hCG concentration to fall by at least 15% during any successive week also resulted in repeated administration of methotrexate. If a repeated dose of methotrexate was given, the day of administration was considered a new day 1. Failure of the serum β-hCG concentration to fall is an indication of salpingectomy.
Results
Between April 2004 and April 2007, 64 women who presented to Al-Hammadi Specialized Hospital, Riyadh, Saudi Arabia, were suspected of having tubal ectopic pregnancies. Hemodynamically unstable patients (6 cases) were subjected to immediate laparotomy and 20 patients received methotrexate as medical treatment for ectopic pregnancy. The remaining 38 patients who were subjected to laparoscopic conservative surgery (salpingotomy) were invited to take part in the trial. Sixteen patients received postoperative methotrexate and were excluded from the study. Twenty-two patients agreed to take part and had a laparoscopic salpingotomy without methotrexate (the study group). Analysis of β-hCG after surgery did not revealed any case of PTT, and none of these patients required methotrexate.
Table 1 shows that, the mean age was 26±5.4 (range 18–41) years, with gravidity between 0 and 6 and parity between 0 and 4. The mean (±standard deviation [SD]) gestational age at diagnosis on the basis of the last menstrual period was 46.8±10.3 days. The maximum diameter of the ectopic mass as measured by sonography was 3.5±1.1 cm, and ranged from 2.0 to 5.0 cm. The amount of intraperitoneal hemorrhage that aspirated at the start of the operation ranged from 110 to 400 mL. The mean preoperative β-hCG concentration was 2847±1544 (range 695–4882) mIU/mL. The β-hCG concentration 2 days postoperatively decreased to ≤50% and after 4 days, <25% of the preoperative level. There was no patient with PTT after linear salpingotomy, and no patient received methotrexate. The postoperative course was uneventful, with no side effects or complications in any women. The follow-up period that patients needed for β-hCG concentration to return to nonpregnant value (<5 mIU/mL) ranged between 10 and 24 days. The maximum time spent in hospital for surgery was 2 days.
Values as mean±standard deviation (SD) (range).
hCG, human chorionic gonadotropin; TVS, transvaginal sonography; mIU, milli-international units.
Discussion
The idea for the present study was to ascertain whether laparoscopic salpingotomy alone without methotrexate can successfully treat a patient with tubal ectopic pregnancy. PTT is associated with persistence of trophoblastic tissue without reduction of the serum β-hCG levels after surgery. The decision to use prophylactic methotrexate must take into consideration if a decrease of >50% on postoperative day 2 and/or a decrease of 75% on postoperative day four is not detected in preoperative serum β-hCG levels.
In the present study, the surgical techniques used during linear salpingotomy included attempted removal of the ectopic pregnancy mass to the greatest possible extent with the least possible traumatizing manipulation, to avoid tubal destruction. In spite of the fact that there is no effective means of predicting which patients will develop PTT, a thorough trial at removing most of the villi can be helped by laparoscopic observation of the lumen of the fallopian tube after the removal to ensure that no villous tissue remains, and copious irrigation with physiologic saline solution. In the present study, PTT was not noted in any of the patients who underwent laparoscopic salpinsotomy for tubal pregnancy. No patient needed methotrexate therapy.
The reported incidence of PTT varies among studies, partly because no standardized definitions have been established. 4 Seifer et al. 7 defined PTT as a morbid state characterized by continuous growth of villous tissue, which needs additional treatment, whereas DiMarchi et al. 17 defined it as a morbid state characterized by postoperative increase of the serum hCG levels or persistence of trophoblastic tissue in the affected fallopian tube. The incidence of PTT following laparoscopy ranges from 3.5% to 20.0%. 18 Pouly et al. 13 achieved a relatively low (3.5%) incidence of PTT in the largest series of patients treated to date by laparoscopic salpingotomy (321 tubal pregnancies), and in many current practices, the incidence of PTT appears to be low. 19
Risk factors for salpingotomy failure and PTT include small ectopic pregnancies (<2 cm diameter), early therapy (<42 days from last menstrual period), and high concentrations of β-hCG (>3,000 mIU/mL) preoperatively that may help guide the decision to administer prophylactic methotrexate after salpingotomy.4,11,12 The likelihood of PTT was significantly increased when the serum β- hCG level increased >40% per day before surgery. 20 However, in practical preoperative examination, tubal pregnancy is sometimes diagnosed by single analysis without repetition. Further, PTT occurred irrespective of the implantation site, including the ampulla, isthmus, or interstitial portion of the fallopian tube. There is a tendency for persistent trophoblastic tissue to be found in the proximal portion of the tube; therefore, special attention to this area is important. 1 Consequently, it is difficult to predict the occurrence of PTT prior to operating for an ectopic pregnancy. 4
A decision analysis study 12 reported that prophylactic methotrexate after linear salpingostomy resulted in 4 ruptured ectopic pregnancies compared with 37 with observation alone (0.4% vs. 3.7%). A total of 19 procedures were performed in the prophylaxis group (4 laparotomies and 15 laparoscopic salpingectomies) as opposed to 47 procedures in the observation group (37 laparotomies and 10 laparoscopic salpingectomies).
Spandorfer et al. 19 reported that <50% reduction of the serum β-hCG level on postoperative day 1 is predictive of PTT, whereas Vermesh et al. 21 reported that a serum β-hCG level >10% of the preoperative level on postoperative day 9 is suggestive of PTT.
Graczykowski and Mishell 22 demonstrated that the rate of PTT was reduced to a rate of 1.9% using methotrexate prophylaxis in comparison with a rate of 14.5% among controls. Spandorfer et al. 20 suggested that if day 1 serum β-hCG concentrations decreased >50% of the preoperative value, there was more than an 85% probability that a PTT would not occur: a drop in β-hCG of <50% was associated with a greater than threefold increased risk of PTT. He also suggested that, when levels declined by at least 77% on postoperative day 1, no PTT occurred. 20 However, to avoid 1 additional case of persistent trophoblast after conservative surgery, 8 women would need to be treated with methotrexate.1,18 Monitoring of the β-hCG concentrations would, therefore, seem to be a better option, provided that the woman was amenable to monitoring. 1 One must, however, never assume that the chance for PTT is entirely mitigated by the characteristics and ease of the procedure. 18
Garcia et al., 12 performed a decision analysis study that reported that prophylactic methotrexate is the optimal treatment as long as certain conditions are met: 1) the incidence of PTT is >9% with salpingostomy alone, 2) the incidence of PTT is <5% when prophylactic methotrexate is given, 3) the probability of ectopic pregnancy rupture is >7.3% with a PTT, and 4) the complication rate associated with methotrexate is <18%. If these conditions are not met, observation without methotrexate becomes the better strategy.
Conclusions
PTT after laparoscopic salpingotomy may be a rare but serious complication. Because PTT cannot be predicted by preoperative features, surgeons should uniformly perform a delicate conservative operation with an attempt at removal of all trophoblastic tissue followed by strict follow-up of serum β-hCG levels, and not to hesitate to give methotrexate if serum β-hCG declines less than expected percentage. The patient group studied here was very small; however, this preliminary experience points to the benefit of methotrexate after salpingotomy for selected cases with suspected PTT.
Footnotes
Disclosure Statement
No competing financial conflicts exist.