
Abstract
Abstract
Introduction
Various techniques have been used to provide adequate hemostasis and minimize blood loss during surgery for placental abnormalities. Endovascular occlusive balloons have been used to reduce the amount of blood loss by occluding the principal vessels supplying the uterus. Prophylactic intraoperative uterine artery embolization is another option, with several reports suggesting favorable results. Many recent reports have been published regarding endovascular procedures concomitant with surgery, with conflicting results in regards to the severity of hemorrhage when compared with traditional surgery.
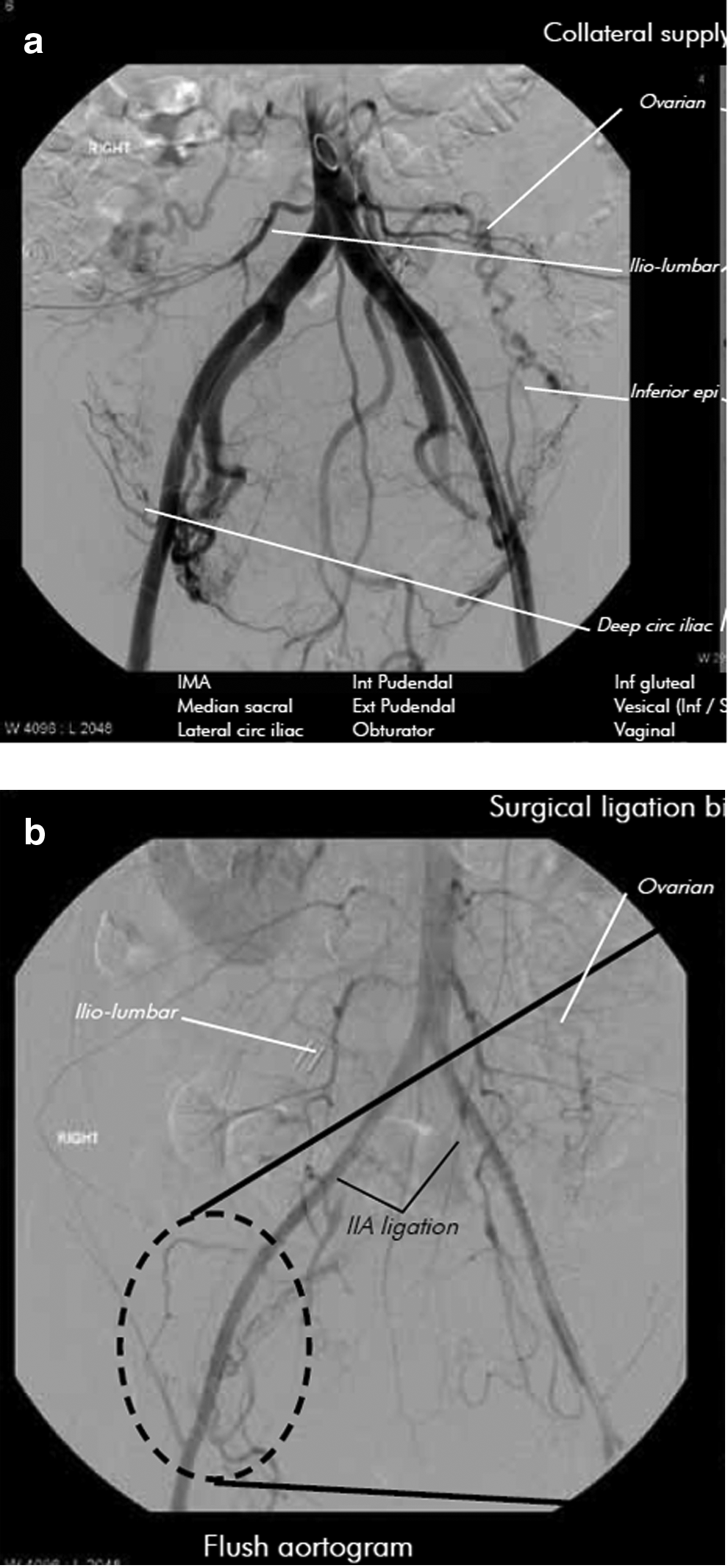
The anatomy of the blood supply to the uterus, with its sources of collateral vessels, explains why adequate hemostasis is challenging in patients with abnormal placentation. The internal iliac artery (IIA) is the main blood supply to the pelvis and is divided into anterior and posterior divisions. The uterine artery, a branch of the anterior division, is the main supply to the uterus (and hence the placenta); however, there are several other vascular territories that provide a rich collateral supply to the uterus. Major anastomoses supplying the IIA after occlusion include aortic branches: ovarian and iliolumbar arteries; and external iliac artery branches: lateral circumflex iliac, inferior epigastric, iliolumbar, obturator and external pudendal arteries. The sources of this collateral circulation have previously been described and it has been hypothesized that a more significant reduction of blood loss can be established through balloon occlusion of the common iliac arteries (CIA) instead of the IIA. 7 There has been a recent angiographic demonstration of the extensive collateral circulation to the placenta from the recruited blood vessels in cases of abnormal placentation (Fig. 1a)with emphasis on the continuous flow in the IIA despite its ligation (Fig. 1b). 8 Physiological studies demonstrated that even after IIA clipping, mean arterial pressure in branches distal to the occlusion was higher than the systemic venous pressure, because of extensive collateral circulation. 9
(
Endovascular management of placenta accreta
The traditional technique to minimize blood loss in patients with placenta accreta has long been surgical ligation of the pelvic arteries. However, this appears to be less effective for controlling postpartum hemorrhage in placenta accreta patients than in other cases with uterine atony, with success rates of <50% in placenta accrete. 10 In addition, surgical ligation takes longer to control bleeding and risks surgical trauma; therefore, the prophylactic use of bilateral hypogastric artery ligation has been found to have limited advantages in the reduction of intraoperative bleeding. 11 Most investigators have suggested a comparable blood flow limiting effect with either surgical ligation or occlusive balloons. This experience has stimulated the emergence of other less invasive and safer techniques to reduce intraoperative blood loss through decreasing pelvic circulation. Occlusive balloons also avert the need for an experienced obstetrician capable of surgically ligating the uterine or IIAs.
The reduction of blood flow obtained by inflating the balloon has the benefit of making the surgical field less bloody and decreasing the risk of iatrogenic damage of other pelvic structures, especially the ureters and bladder. 12
During a cesarean delivery, balloons are only inflated after delivery of the newborn to avoid the risk of placental ischemia before delivery. Most studies have used the IIA, the anterior division of the IIA, or the uterine artery as sites for balloon occlusion. Another site for balloon occlusion is the CIA, which can only be kept inflated for short intervals, to reduce the risk of leg ischemia. The abdominal aorta is an alternative site proposed for occlusion. There are a total of 5 reported cases using the infrarenal abdominal aortic position for balloon occlusion, which were described over a 15 year interval.13–18 The procedure is relatively easy, as the balloon can be placed in a short amount of time because a single catheter insertion is sufficient, unlike the IIA and CIA where bilateral balloon placement is needed. There is no need for contrast injection and radiation exposure is minimal.
Moreover, endovascular catheterization has the added benefit of preserving future fertility, by having the patient undergo selective embolization, to prevent hysterectomy. Uterine artery embolization has been developed as a first-line alternative treatment for patients with postpartum hemorrhage refractory to medication. 18
Guidelines of the Royal College of Obstetricians and Gynaecologists (RCOG) recommend the use of interventional radiology to minimize blood loss in elective surgery and emergent cases of abnormal placentation, by inflating occlusive balloons in the IIA or uterine artery. 19 However, the American Congress of Obstetricians and Gynecologists (ACOG) recently updated its guidelines and only briefly mention adjuvant embolization as an option.
In this study, literature regarding the use of endovascular balloon occlusion and the outcomes were reviewed, in addition to a proposed outline for future management.
Materials and Methods
A systematic MEDLINE search was performed to identify studies addressing the outcome of intravascular occlusive balloons to decrease blood loss in patients with abnormal placentation, compared with conventional surgery alone. All articles in the English language from 1995 through 2011 were included. The key words used were abnormal placentation, internal iliac occlusive balloons, placenta accreta, and uterine embolization. References from the articles were also searched for the key terms. The studies were reviewed for site of occlusion and for outcomes in blood loss, blood transfused, length of surgery, length of hospital stay, and final outcome.
Results
This review included all reports that used balloon catheters with and without embolization. There were 19 studies in the period between 1995 and 2011. The review included 57 cases with a mean age of 33.9 years. There were 5 cases with balloon placement in the anterior division of the internal iliac artery, 2 cases of balloon inflation in the common iliac artery, 3 cases of balloon inflation in the infrarenal abdominal aorta, and in the remaining 47 cases, the balloons were inflated in the IIA. Three studies used arterial embolization in addition to balloon occlusion.20–22 All 19 studies are summarized in Table 1.
Fuller AJ, Carvalho B, Brummel C, Riley ET. Epidural anesthesia for elective cesarean delivery with intraoperative arterial occlusion balloon catheter placement. Anesth Analg 2006;102:585.
Mushtaq S, Kurdi W, Al-Shammari M. Prophylactic catheters placement and intraoperative internal iliac artery embolisation in a patient with placenta accreta. J Obstet Gynaecol 2007;27:853.
Yi KW, Oh MJ, Seo TS, So KA, Paek YC, Kim HJ. Prophylactic hypogastric artery ballooning in a patient with complete placenta previa and increta. J Korean Med Sci 2010;25:651.
Russo M, Krenz EI, Hart SR, Kirsch D. Multidisciplinary approach to the management of placenta accreta. Ochsner J 2011;11:84.
EBL, estimated blood loss; IIA, internal iliac artery; IIAOBC, internal iliac artery occlusive balloon catheter; CIA, common iliac artery; CIAOBC, common iliac artery occlusive balloon catheter.
Occlusion of the infrarenal abdominal aorta has been reported for >15 years, usually after urgent intraoperative insertion of the occlusive balloon. The first mention, initially proposed by Paull et al. in 1995, showed favorable results. 13 In 2003, Bell-Thomas et al. reported the emergency use of a transfemoral 10-French aortic occlusion catheter to control massive bleeding in a patient with placenta percreta. 14 This was better demonstrated by Masamoto et al. in 2009, when an aortic balloon catheter was inflated for 80 minutes and Doppler ultrasonography of the placental site demonstrated an abrupt decrease in blood flow. 15 In 2011, Andoh et al. also used prophylactic abdominal aortic occlusion in a patient with placenta accreta and suggested that it is a safe and effective method. 16 Three publications demonstrated the use of the CIA for balloon occlusion and all three showed favorable outcomes.7,23,24 In a case series of 62 patients by Miller et al., blood loss during cesarean hysterectomy associated with placenta accreta without use of endovascular balloons or occlusive devices was quantified. 25 Estimated blood loss exceeded 2 L in 41 patients, 5 L in 9 patients, 10 L in 4 patients, and 20 L in 2 patients. Blood transfusion was required in 32 patients and blood product replacement ranged from 5 to 70 units. In 3 patients, ureteral transection and reimplantation was performed. Additional surgical complications were distributed among 7 patients, but there were no maternal deaths. In comparison, an evaluation of data from the cases reported in Table 1, with use of balloons, showed that the mean blood loss was 3.15 L; the reported mean blood transfused was 7.2 units, and the mean hospital stay was 6.2 days.
Controlled study outcomes
There were only five case controlled studies that compared hysterectomies with or without occlusive endovascular balloons; patient characteristics, blood loss, and complications for these five studies are described in Table 2. Of the five studies, two showed favorable outcomes with occlusive balloons prior to surgery;24,26 the remaining three studies27–29 showed no significant difference in outcome between the two procedures. A study of 9 patients by Levine et al. was prospective, 29 whereas the other four studies (Shrivastava et al., Bodener et al., Tan et al., and Angstmann et al.) were retrospective.24, 26–28
EBL, estimated blood loss; ICU, intensive care unit; CAI, common iliac artery; IIA, internal iliac artery.
Angstmann et al. and Tan et al. both noted statistical significance for less intraoperative blood loss (p=0.0001 and p=0.042 respectively) and fewer blood units transfused (p=0.013 and p=0.005 respectively) between cases with and without endovascular balloons. Angstmann et al. observed a significant difference in the amount of blood loss in the 8 cases of staged embolization compared with conventional techniques (553 mL vs. 4517 mL, p=0.0001). Whereas the study by Tan et al. noted a significantly shorter operative time in the balloon group (p=0.046), Angstmann et al. showed similar operating times in both groups and significantly longer anesthetic times in the balloon group (6.59 hours vs. 2.67 hours, p=0.0001). Angstmann et al. also reported fewer intensive care unit (ICU) admissions (1 in the staged procedure group vs. 7 in the surgery group) and a shorter length of postoperative hospital stay, although not statistically significant (p=0.107). There were no endovascular catheter related complications in either study. Balloons were inflated in the CIAs and the IIAs in the studies by Angstmann et al. and Tan et al., respectively.
The largest study comparing these two treatment modalities for placenta accreta was that conducted by Shrivastava et al., which comprised 69 patients. The two studies by Shrivastava et al. and Bodener et al. revealed no statistical significance between groups regarding intraoperative blood loss (p=0.79 and p=0.4, respectively), amount of blood transfused (p=0.6 and p=0.47 respectively) and operative time (p=0.85 and p=0.052 respectively). Shrivastava et al. and Levine et al. showed no significant difference between comparing length of hospital stay (p=0.85 in Shrivastava et al.). The study by Bodner et al. showed that the balloon occlusion plus embolization group had a statistically significant longer hospital stay; 23 days in the balloon group versus 8.8 days in the surgery group (p=0.007).
Discussion
Among the controlled studies, four studies (Tan et al., Shrivastava et al., Levine et al., Bodner et al.) placed the occlusive balloons either in the IIA, anterior division of the IIA, or, less commonly, in the uterine artery. Three of these studies reported no statistical differences in blood loss, operative time, or length of hospital stay between the balloon occlusion group and the standard surgical group. The continuing high collateral blood flow when the occlusive balloons were inflated in such a distal location may explain why in some studies no added benefit was noticed when using IIA occlusive balloon catheters. IIA occlusive balloon catheters (IIAOBC) do not completely abolish blood flow to the uterus because of the rich collateral vessels, although some reports have confirmed that pulse pressure distal to the site of obstruction is reduced. 30 In contrast, the study by Angstmann et al. described placing the occlusive balloons in the CIA instead of the IIA, which may explain the decrease in maternal morbidity in this group. Radiologists occasionally use the CIA instead of the IIA for several theoretical and practical benefits. First, occluding this more proximal site would abolish the collateral supply reaching the IIA through the branches of the external iliac artery, thereby potentially providing better hemostatic results. Another benefit of the CIA balloon catheter is the ease of deployment of the catheter within this location, especially for those cases with unusual vascular anatomy. The procedure time and radiation exposure are decreased, and contrast medium is either not required or is greatly reduced. Selective embolization of the entire uterus and placental bed was performed in 8 cases in the study by Angstmann et al., and demonstrated statistical significance in blood loss between both groups. 24 In the study by Bodner et al., the embolization group also had a longer hospital stay compared with the conventional surgery group, 27 because the embolization group was hospitalized for a longer period of time prior to surgery (i.e., because of factors unrelated to balloon placement). In the study by Shrivastava et al., there were three catheter-related complications; 1 patient had an IIA thrombosis and groin hematoma, another patient had an IIA dissection with 80%–90 % occlusion, and a third patient had a femoral artery thrombosis. The second and third patients had iliofemoral bypass surgery because of the persistence of their symptoms.
Out of the 19 cases reports and case series, 13 showed favorable outcomes for occlusive balloons, whereas 6 studies were associated with complications. Most of these were vascular complications related to the balloon catheters. Mok et al. concluded that there was no added benefit for occlusive balloons, and suggest that balloons do not seem to reduce the need for cesarean hysterectomy. 31 In the article by Sewell et al., 32 the case was complicated by a postoperative popliteal artery embolus requiring embolectomy. The study by Greenberg et al. was complicated by left lower limb ischemia caused by left iliac thrombosis. 33 The study by Bishop et al. was complicated by pseudoaneurysm, unilateral arterial rupture, and acute right lower limb ischemia requiring thrombectomy. 34 In his case series of 14 patients, Thon et al. described 4 patients with complications, 1 patient had massive hemorrhage leading to cardiac arrest, and all 4 required intervention for catheter-related complications. 35
Two patients in whom CIA occlusion was used,7,23 and the 3 patients in whom aortic occlusion was used13–15 had a favorable outcome. With the favorable outcome reported with aortic cross-clamping in surgeries for abdominal aortic aneurysms, authors recommending aortic occlusive balloons have deemed this procedure relatively safe, because of the rich collateral web during pregnancy, in addition to the absence of complete occlusion of blood flow by the balloon catheter. A technique adopted by Chou et al. is the temporary cross-clamping of the infrarenal abdominal aorta for a duration of 1 hour in a patient with placenta accreta. This was reported to result in a sudden and dramatic reduction in blood loss. 17 Although these results are promising, larger case series are needed to assess the safety and effectiveness of this procedure.
As demonstrated, most of the published reports used the IIA as the occlusion site, leaving the rich placental collateral circulation to continue feeding the placenta and possibly contributing to the continued bleeding after balloon inflation. The alternative use of the CIA may greatly diminish the collateral supply. Although this level of occlusion carries a risk of potential lower limb ischemia, because of occlusion of flow to the lower extremities. Methods to decrease this risk include short balloon inflation time (∼20 minutes) when the balloon is only inflated after delivery of the fetus, deflation of the balloon for short periods between inflations, and monitoring lower extremities for any signs of ischemia by placing pulse oximetry and/or an arterial line. Prolonged surgeries can carry a substantial risk if balloons are kept inflated for longer durations in the CIA.
The main complications with occlusion of the CIA are distal ischemia, reperfusion injury, thrombosis, and/or embolism of the lower extremities, which receive their supply through the external iliac artery. However, these complications can be avoided by limiting the occlusion time as much as possible, placing the balloons immediately prior to planned surgery and, if feasible, administering a small dose of heparin to avoid catheter-related thrombosis and/or embolism. Occlusion of the abdominal aorta also carries risks. The major complications are aortic rupture, atheroemboli with distal ischemia, reperfusion injury caused by prolonged aortic occlusion, and either thrombosis or embolism. Risks of embolization include unexpected late complications such as pelvic pain, sexual dysfunction, or bladder ischemia. 23
This review found that the case reports and case series noted less morbidity in patients who had occlusive balloons prior to surgery. In most of these cases there were minimal complications. However, when the endovascular balloon group was compared with the conventional surgery group in the five studies in Table 2, results were conflicting. There were particularly conflicting results when the balloons were placed in the IIA, but when placed in the CIA, results were more consistent. The series of patients receiving aortic occlusion in the five published case reports seemed to have more positive outcomes. It can therefore be concluded that the success rate in blood sparing is directly proportional to the amount of available collateral circulation. In other words, the higher the occlusion level, the better the outcome. In total, 200 patients were evaluated in these reports, showing no mortality; this result is comparable with the extensive report by Gielchinsky et al. of 310 patients with placenta accreta, which reported only one maternal mortality. 36
Embolization of the uterine artery to occlude placental vessels and reduce possible hemorrhage has been less often described than intravascular balloons. Whereas the overall incidence of embolization failure is ∼5%, >50% of these cases fail because of placenta accreta, increta, or percreta. 37 It is hypothesized that the cause of failure of embolization is vascular spasm that occurs because of massive blood loss. 38 To avoid spasm of the uterine artery, Bodner et al. preferred placing the occlusive balloons in the anterior division of the IIA to embolize. 27 Further studies to observe the outcome of uterine artery embolization versus conventional approach are necessary.
By analyzing the design and outcome of these studies, it is noticeable that all of the studies comprise a small number of patients, affecting the statistical power of these results. Therefore, there is a need for a multicenter randomized case control study to collect data from a larger patient population. Among the five studies described in Table 2, all operative procedures were not performed by a single obstetrician, increasing the variability of the results. In the study by Angstmann et al., 3 different gynecologic oncologists performed the surgeries. The other four studies did not mention the number of surgeons involved in these procedures.
Future studies should be randomized according to the site of occlusive balloons (e.g., IIA vs. CIA) and illustrate the relationship between site of balloon occlusion and outcome.
Referral to large institutions with centralization of resources will increase the quality of care in the future and will allow the concentration of multiple experts required to manage the rare but complex condition of placenta accreta. The best result will be achieved when there is a large group of specialists available, including interventional radiologists, pelvic surgeons, expert obstetric and gynecologic surgeons, perinatologists, intensivists, and anesthesiologists who are experts in massive blood resuscitation, all using stringent care protocols.
Increasing the availability of the endovascular operating suites (hybrid suites that provide both endovascular and operating room capabilities) in the hospital will reduce patient transportation between the radiology suites and the operation room and also reduce procedure time, thereby limiting catheter-related complications, decreasing radiation exposure, and allowing for immediate emergent embolization in cases of uncontrollable bleeding after delivery. It is also important to realize that there should be a multidisciplinary team, in order to minimize morbidity and mortality in these cases.
Conclusions
In conclusion, a review on outcomes in management of placenta accreta with either staged occlusive endovascular balloons with and without embolization followed by surgery versus conventional surgery alone, is presented. The data presented support the utility of the endovascular approach, despite a relative paucity of data resulting from the rarity of the condition. There may also be a bias toward reporting only well-managed cases. Despite this, the most organized teams have been able to use intravascular balloon obstruction and embolization to minimize or
Footnotes
Disclosure Statement
No competing financial interests exist.