
Abstract
Abstract
Introduction
Epithelial proliferations have been considered to be benign tumors of the uterine tube and are occasionally found during the microscopic examination of a specimen of tubal ligation or salpingectomy by some, whereas such proliferative epithelial lesions have been called “adenomatous hyperplasia” (ATH) or “carcinoma in situ” by others.2–4 These have also been divided into three groups: benign tubal hyperplasia (BTH), ATH, and CIS. 4 The frequency with which these proliferative epithelial lesions are found and the rarity of invasive carcinoma of the uterine tube makes it extremely unlikely that these represent noninvasive carcinoma, and they may, in fact, represent a “field effect” hypothesized.5,6
An association of tubal epithelial proliferation with lesions in other areas of the genital tract and exogenous and endogenous estrogen stimulation has been demonstrated. 4 Tubal epithelial proliferations have been described by Moore et al. 5 in association with salpingitis, endometrial hyperplasia, adenocarcinoma of the uterus, endometritis, deciduas of pregnancy, effect of oral contraceptive pill (OCP), and irradiation necrosis. Others have documented such association with uterine fibromyoma, benign/malignant ovarian tumors, serous borderline tumors of the ovary, hormone-producing ovarian tumor, and leiomyosarcoma.3,4,7 However, progression of these proliferative lesions to invasive tubal cancer was not documented.3,4
Association of proliferative epithelial lesions of the uterine tube with lesions of the ovaries has been variously described.4,5,8 These lesions may be easily confused with CIS of uterine tube, from which they must be differentiated. In a patient with a proliferative epithelial abnormality in the uterine tube who had undergone hysterectomy, the associated inflammatory, neoplastic, or hormonal lesions in the ovaries may be apparent and correlated.4,5
In the light of the available literature, this study planned to examine the proliferative epithelial lesions of the uterine tube and their association with ovarian pathologies.
Materials and Methods
A total of 62 panhysterectomy or hysterectomy with unilateral salpingo-oophorectomy specimens, with primary lesion in the ovaries, sent to the Department of Pathology, constituted the material for the present study. On being received, the specimen was cut as per the routine and kept overnight for fixation. Thereafter, in addition to the routine pieces of corpus uteri, cervix uteri, and ovaries, as dictated by the pathologic process present, each uterine tube was blocked for microscopic sections. The conventional hematoxylin and eosin stained microsections prepared from the specimen were extensively studied and, wherever necessary, special stains were used. The findings so obtained were analyzed and correlated with diseases of the ovary as well as with coexistant tubal lesions.
The histologic changes in the uterine tubes were studied for one or more of the following characteristics as advocated by Moore and Enterline: nuclear crowding, stratification of nuclei, loss of polarity, nuclear atypia, mitoses, papillae (papillary formation), solid proliferation, inflammation and acidophilic metaplasia. 5
The three groups of epithelial abnormalities as per the criteria adopted by Stern et al. are shown in Table 1. 4
BTH, benign tubal hyperplasia; ATH, atypical tubal hyperplasia; CIS, carcinoma in situ.
Observations
The present study was conducted on 62 cases of panhysterectomy or hysterectomy with unilateral salpingo-oophorectomy, with primary lesion in the ovaries. Of these 62 cases, panhysterectomy specimens were received in 56 cases and hysterectomy with right and left salpingo-oophorectomy accounted for 3 cases each. Therefore, in 62 cases, a total of 118 uterine tubes were studied. Most patients were between 41 and 50 years of age. The youngest patient was 22 years old and oldest patient was 70 years old.
There were 22 cases of benign surface epithelial tumors of ovaries out of which 6 showed associated lesions in other parts of genital tract. Three cases showed leiomyoma, two salpingitis, and one endometrial hyperplasia. Out of 19 cases of malignant surface epithelial tumors, associated lesions in other parts of the genital tract were seen in 12 cases, out of which in 8 cases secondary tumor deposits were seen in the uterine tubes. Three cases also showed associated uterine leiomyoma; two cases each showed endometrial hyperplasia and leiomyoma. One out of seven cases of sex cord stromal tumors showed associated endometrial hyperplasia. Two out of 10 cases of germ cell tumors showed leiomyoma, and 1 case showed associated salpingitis. In all the three cases of oophritis, salpingitis was also seen, and 2 cases also had leiomyoma. One case showed borderline surface epithelial tumor of serous type (Table 2).
15 serous, 6 mucinous, and 1 endometrioid cystadenoma.
5 papillary serous cystadenocarcinomas, 6 papillary adenocarcinomas, 3 adenocarcinomas, 3 mucinous adenocarcinomas, 1 endometrioid adenocarcinoma, and 1 malignant Brenner.
4 granulosa cell tumor, 2 fibromas and 1 unclassified malignant sex cord stromal tumor.
9 teratomas and 1 endodermal sinus tumor.
Of the 118 uterine tubes (62 cases) studied, 82 tubes showed tubal epithelial proliferation, out of which most, 56 (47%) showed BTH, whereas 8 (7%) revealed ATH, and 18 (15%) showed CIS; 36 (31%) showed normal tubal epithelial morphology (Table 3). The histologic pattern of uterine tubal epithelium was similar bilaterally in 53 (95%) cases out of 56 cases of panhysterectomy. In the remaining 3 (5%) cases, histologic pattern of uterine tubal epithelium was bilaterally dissimilar.
Histologic pattern of uterine tubal epithelium with associated lesions in ovaries
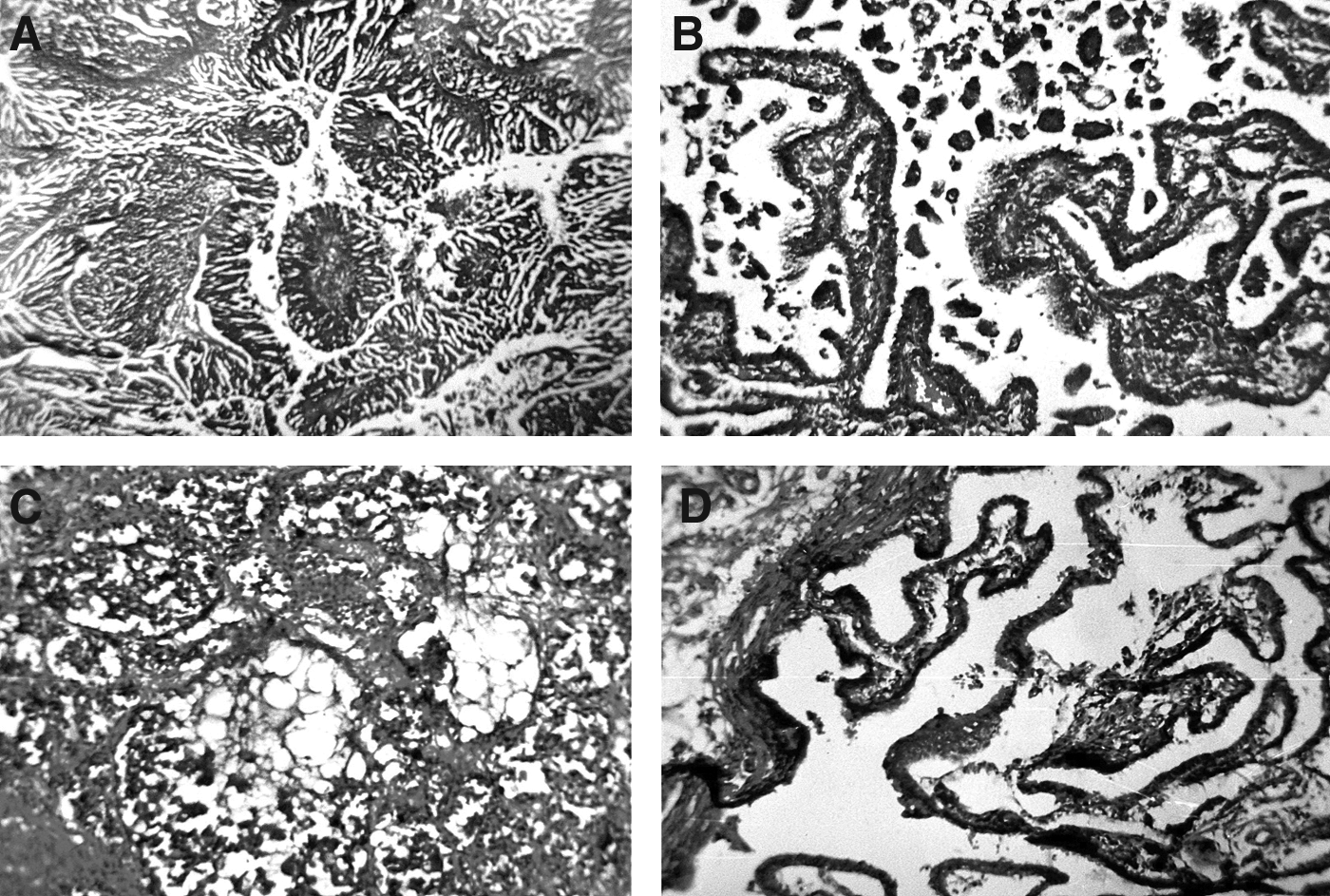
Out of 22 cases of benign surface epithelial tumors, 13 cases (59%) showed proliferative epithelial lesions of the uterine tube of the BTH type and the remaining 9 cases had normal tubal morphology. Out of 19 cases of malignant surface epithelial tumors, proliferative epithelial lesions of the uterine tube were seen in 15 cases (79%), which were more prevalent and were of higher grade, that is, ATH/CIS, in 47.4% of cases, including those showing secondary deposits in tubes (Fig. 1).
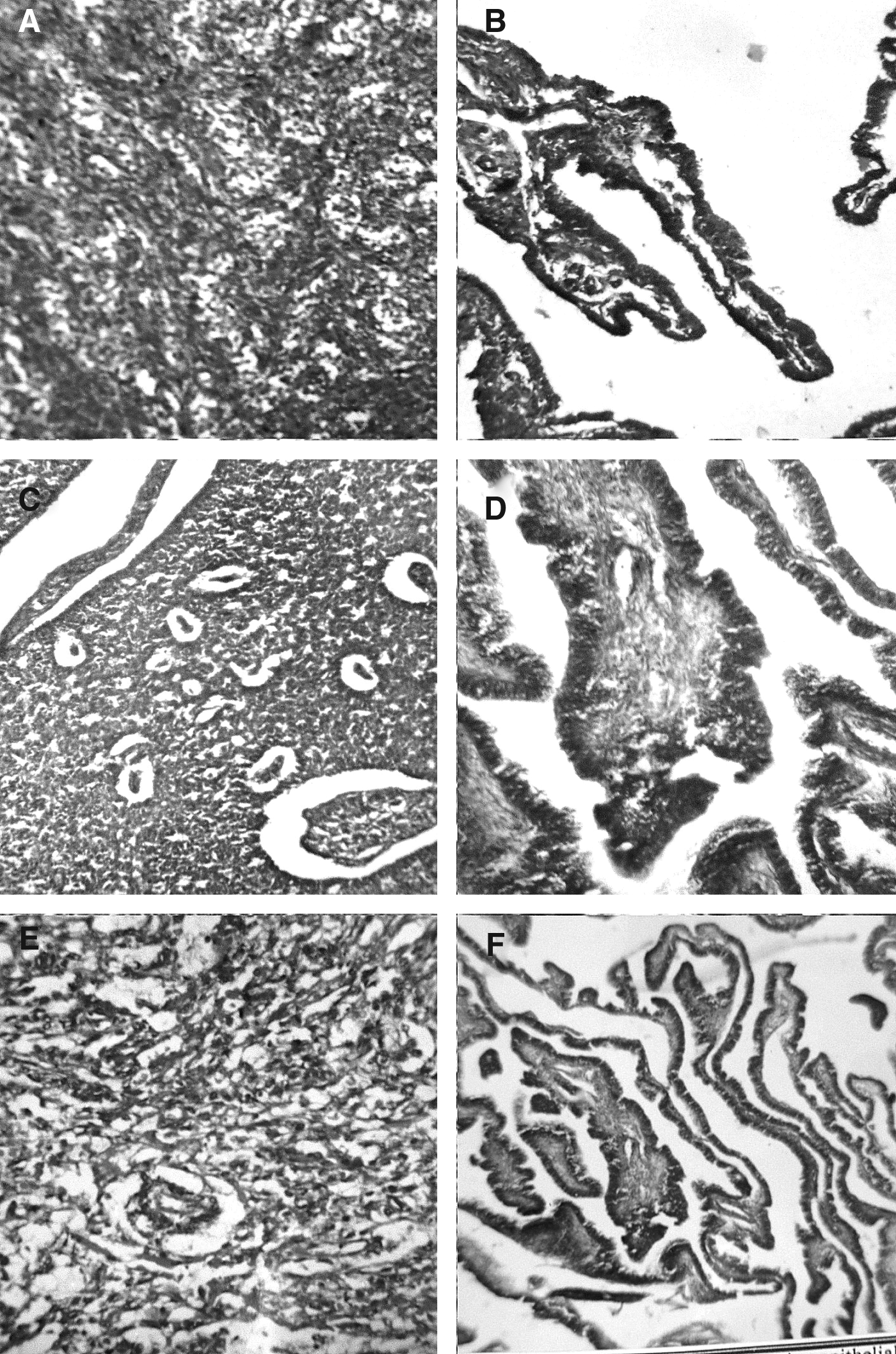
All the seven cases of sex cord stromal tumors (4 granulosa cell tumor, 1 unclassified malignant sex cord stromal tumor, and 2 fibromas) and associated lesions, showed proliferative epithelial lesions of the uterine tubes of varying degrees, that is, BTH (4 cases), ATH (1 case), and CIS (2 cases). Three cases with ATH/CIS were of granulosa cell tumor (Fig. 2).
Malignant tumors of the ovary (nonepithelial) with corresponding lesions in the fallopian tubes (
Five out of 10 cases (50%) of germ cell tumors and associated lesions, 2 out of 3 cases (66.7%) of oophritis, and 1 case (100%) of borderline epithelial tumor showed proliferative epithelial lesions of the uterine tubes of varying severity (Table 4).
15 serous, 6 mucinous, and 1 endometrioid cystadenoma.
5 papillary serous cystadenocarcinomas, 6 papillary adenocarcinomas, 3 adenocarcinomas, 3 mucinous adenocarcinomas, 1 endometrioid adenocarcinoma, and 1 malignant Brenner.
4 granulosa cell tumor, 2 fibromas, and 1 unclassified malignant sex cord stromal tumor.
9 teratomas and 1 endodermal sinus tumor.
BTH, benign tubal hyperplasia; ATH, atypical tubal hyperplasia; CIS, carcinoma in situ.
Proliferative epithelial lesions of one type or another were found in the great majority of cases with a lesion in the ovaries, varying from 50% (with germ cell tumors) to 100% (with sex cord stromal tumors). In cases with proliferative lesions, all cases (100%) of benign surface epithelial tumors and borderline surface epithelial tumor of the serous type were associated with benign hyperplasia; whereas lesions were of high grade (ATH and CIS) when found in association with malignant surface epithelial tumors.
Results
Tubal epithelial proliferation has received relatively scant attention in the gynecologic pathology literature. Some investigators claim it to be an uncommon finding that has a particular association with a number of neoplastic and pre-neoplastic lesions of the female genital tract, whereas others believe that tubal epithelial proliferation especially of mild degree (BTH) is found in direct proportion to the diligence exercised in searching for it, and that it is usually an incidental and focal finding with no special clinical significance.4–6,9 However, it has become a focus of greater attention during the last few years, after the recognition of its role in the development of serous carcinoma in women with germline BRCA mutations who undergo risk-reducing salpingo-oophorectomy.10,11 Recent contributions have progressively pinpointed the tubal epithelium as the potential origin of tubal, ovarian, and peritoneal carcinomas, not only in the BRCA mutation setting but also in sporadic adnexal epithelial tumors.12–14 This knowledge has led pathologists to heighten their index of suspicion regarding tubal atypia and has resulted in an appreciation of subtle neoplastic changes occurring in the fallopian tube epithelium, as well as the propensity of reactive atypia to mimic serous CIS. 15 The prevalence and clinical significance of mucosal epithelial proliferation (MEP) or hyperplasia of the fallopian tube are controversial in the few studies reported, and there are differing opinions about its significance and importance. 16 The presence of hyperplastic tubal mucosal lesions that are occasionally difficult to differentiate histologically from adenocarcinoma in cases of chronic salpingitis has been reported for many years, and was recently re‐emphasised by Cheung and colleagues. 17 Piek et al. concluded that hyperplastic/dysplastic changes in the epithelium of uterine tubes were common in women predisposed to developing ovarian carcinoma, whereas Crum supported the data that the distal fallopian tube is an important site for serous carcinogenesis, stressing both the presence of a novel precursor (p53 signature) and the application of this model to all women irrespective of BRCA status.18,19 Kurman proposed that ovarian low-grade serous proliferations are also derived from papillary tubal hyperplasia, which appears to be induced by chronic inflammation. 20
The present study discusses proliferative epithelial lesions of the uterine tube and their association with lesions in the ovary in 62 cases of panhysterectomy or hysterectomy with unilateral salpingo-oophorectomy.
Of the 62 cases, 56 cases (90%) were of panhysterectomy and remaining 6 cases (10%) were of hysterectomy with unilateral salpingo-oophorectomy. Most patients were in the perimenopausal age group, that is, 41–50 years (58%). The cases were distributed according to the type of ovarian lesions—inflammatory or neoplastic (benign/malignant)—and were evaluated for the presence of proliferative epithelial lesions of the uterine tube/s, which were categorized into BTH, ATH, or CIS, as per the criteria adopted by Moore et al and Stern et al.4,5
Incidence of proliferative epithelial lesions of the uterine tube
Out of a total of 62 cases, 43 cases (69%) (41 panhysterectomy, 2 panhysterectomy with unilateral salpingo-oophorectomy) showed tubal epithelial proliferation of one type or the other. The proliferative epithelial lesions were bilaterally similar in 37 out of 41 cases (90%) of panhysterectomy. Yanai-Inbar et al. also observed no major difference in the proportion of bilaterality in different diagnostic categories. 1 In 18 cases, normal tubal histologic pattern was present, and this was mainly observed in cases with benign cystic teratoma and serous cystadenoma.
A wide variation in the incidence and prevalence of proliferative epithelial lesions of the uterine tube has been reported in literature. Moore and Enterline observed a 19% incidence of tubal epithelial proliferation, Bannatyne and Russell found it to be ∼ 60%, whereas the findings of Yanai-Inbar et al. were much higher, being 83%.1,5,21 Our results are almost similar to the ones reported by Bannatyne and Russell. 21
Distribution of tubal epithelial abnormalities in different histopathologic groups
Out of 118 tubes studied, proliferative epithelial lesion was present in 82 (69%) (43 cases) of them. We observed BTH in 28 cases (65%), ATH in 5 (12%), and CIS in 10 (23%), highlighting that BTH was the most common morphologic alteration observed. Stern et al. in their study on tubes from selected hysterectomy specimens found BTH in 22%, ATH in 26%, and CIS in 49%, whereas Yanai-Inbar et al. graded the lesions as mild, moderate, and marked MEPs and observed that mild epithelial proliferation existed in most cases, that is, 52.8%; moderate in 26.7% and severe in 3.14%.1,4
In this study, BTH was maximally observed in benign conditions such as benign cystic teratoma and serous cystadenoma, whereas ATH/CIS were seen in malignant neoplasms. This study's findings are in concordance with those of Yanai-Inbar et al., who stated that a mild degree of epithelial proliferation is of not much clinical significance, and it is the moderate to marked epithelial proliferation that should be considered as a diagnosable lesion. 1
Association of tubal epithelial abnormalities with ovarian lesions
Of the 62 cases, 33 cases (53%) were of benign ovarian tumors, 25 cases (40%) were of malignant ovarian tumors, and 1 case was of borderline surface epithelial tumor of the serous type. The remaining 3 cases were of oophritis. Proliferative epithelial lesions of the uterine tube were seen in 69% of cases.
Out of 33 cases of benign ovarian tumors, tubal epithelial proliferation was seen in 19 cases (57.5%); BTH in 54.5%, and CIS in 3% of this group as a whole. Out of 25 cases of malignant ovarian tumors, proliferative lesions were seen in 21 cases (84%), and on further analysis of the total cases of this class, lesions were found to belong to BTH in 36%, ATH in 12%, and CIS in 36%. One case of borderline serous epithelial tumor showed proliferation of the BTH type.
Discussion
From the preceding data, it is evident that BTH was mainly observed in cases of benign ovarian tumors, whereas ATH and CIS were more frequently seen to be associated with malignant ovarian tumors. In 43 out of 62 cases in which tubal epithelial proliferation was observed, ATH coupled with CIS was a very conspicuous finding in 9 out of 15 cases of malignant surface epithelial tumors, 3 out of 7 sex cord stromal tumors, 1 case of germ cell tumor (benign cystic teratoma), and 2 cases of oophritis.
A wide variation in the incidence and prevalence of proliferative epithelial lesions as a whole as well as of different types and severity has been reported. Therefore, whereas Moore et al. emphasized that changes in the uterine tubes observed by them did not suggest any association of carcinoma of the ovary with endosalpingeal epithelial abnormality; Bannatyne et al. concluded that MEP of all shades, that is, hyperplasia, dysplasia, or CIS could be found with approximate equal frequency in association with serous, mucinous, and endometrioid tumor and fibromas, and with malignant, proliferating, and benign tumors.5,21 Robey and Silva, on the contrary, have brought out a particular association of tubal epithelial proliferation with low malignant potential (LMP) tumor of the serous type. 7 In an attempt to further extend these observations and to specifically confirm or refute the hypothesis of a specific association of tubal epithelial hyperplasia with ovarian serous neoplasms, Yanai-Inbar et al. concluded that ovarian, endometrial, and cervical carcinoma taken together yielded a prevalence of moderate to marked MEP of the tube that was nearly identical to that with serous LMP tumors, but with the difference that MEP tended to be more widespread and mitotically active. 1 Taking together all shades, MEP of the tubal epithelium were observed in 69% of the cases of ovarian pathology in this study, which percentage is closest to, but slightly higher than, that observed by Bannatyne et al. 21
ATH and CIS taken together were a conspicuous feature with malignant surface epithelial tumors followed by sex cord stromal tumors, and in cases of oophritis. The findings of this study tended to indicate an association of tubal epithelial hyperplasia of moderate to marked severity with malignant surface epithelial tumors of the serous type, and they derive support from the observations of Robey and Silva. 7 To be more precise, however, this study's findings are in full consonance with the observations of Yanai-Inbar et al., who observed such tubal epithelial proliferations of moderate to marked degree in association with nonserous tumors that were nearly identical to those associated with serous tumors, and the findings of Bannatyne et al., who observed tubal epithelial proliferation with almost all types of benign and malignant tumors of the ovary.1,21 The one case of benign cystic teratoma showing tubal epithelial proliferation of the CIS type in this study looked somewhat paradoxical. especially in view of the general trend as brought out in the preceding discussion on ovarian tumors. Such an association can exist, and is supported by the observation of Blaustein, who in addition to benign germ cell tumor, had reported tubal adenocarcinoma, even in association with mixed mesodermal tumors of the uterus. 22
Based on current knowledge, such tubal proliferation may not be tubal carcinoma but severe or marked epithelial proliferation, which corresponds to CIS changes observed in this study.
It is conceivable that when the irritant is sitting at close quarters, proliferative epithelial changes are expected. Tubal epithelial proliferation in cases of oophritis were observed in 2 out of 3 cases, which were not divorced from salpingitis, and such findings are explained on the basis of earlier observations made by Dougherty et al., Pauerstein et al., Moore et al., and Yanai-Inbar et al.1,5,6,23
Crystallizing the discussion on different study groups with available literature in the preceding paragraphs, a further attempt has been made to see the proliferative lesions in benign/ inflammatory and malignant lesions of the ovary (Table 5). Out of the total 36 benign/inflammatory cases, proliferative lesions were seen in 21 (58.3%) cases and further analysis revealed that the cases belonged to BTH in 19 (52.7%), ATH in 1 (2.8%), and CIS in 1 (2.8%) highlighting that BTH was the most common morphologic alteration seen, whereas ATH and CIS were less common. This finding is consistent with the observations made by Yanai-Inbar et al. 1 The remaining 26 cases had borderline/malignant lesions, of which epithelial proliferation was seen in 22 (84.6%) cases. They were further categorized as BTH in 10 (38.4%) cases, ATH in 3 (11.6%), and CIS in 9 (34.6%). This clearly states that ATH and CIS together accounted for>50% of the cases of proliferative epithelial lesions in association with ovarian invasive cancers. These findings are similar to the ones reported by Stern et al. and Yanai-Inbar et al.1,4
PEL, proliferative epithelial lesion; BTH, benign tubal hyperplasia; ATH, atypical tubal hyperplasia; CIS, carcinoma in situ.
Conclusions
Proliferative epithelial lesions of varying degrees were seen in association with various neoplastic (benign and malignant) and inflammatory lesions of the genital tract, but ATH and CIS (moderate to severe) were seen in association with malignancies in the ovary. ATH and CIS should be considered as distinct clinical entities. Primary/premalignant proliferative epithelial lesions of the uterine tube, if diagnosed in isolation, should be viewed with considerable caution and need thorough investigation to prove or rule out concomitant pathology, this being consequent to some precipitating lesions present in the ovary.
Footnotes
Acknowledgment
The authors acknowledge the contribution of Dr. Rajeev Sen, Senior Professor and Head, Department of Pathology, PGIMS Rohtak. in preparation of the manuscript.
Disclosure Statement
No competing financial conflicts exist.