
Abstract
Abstract
Introduction
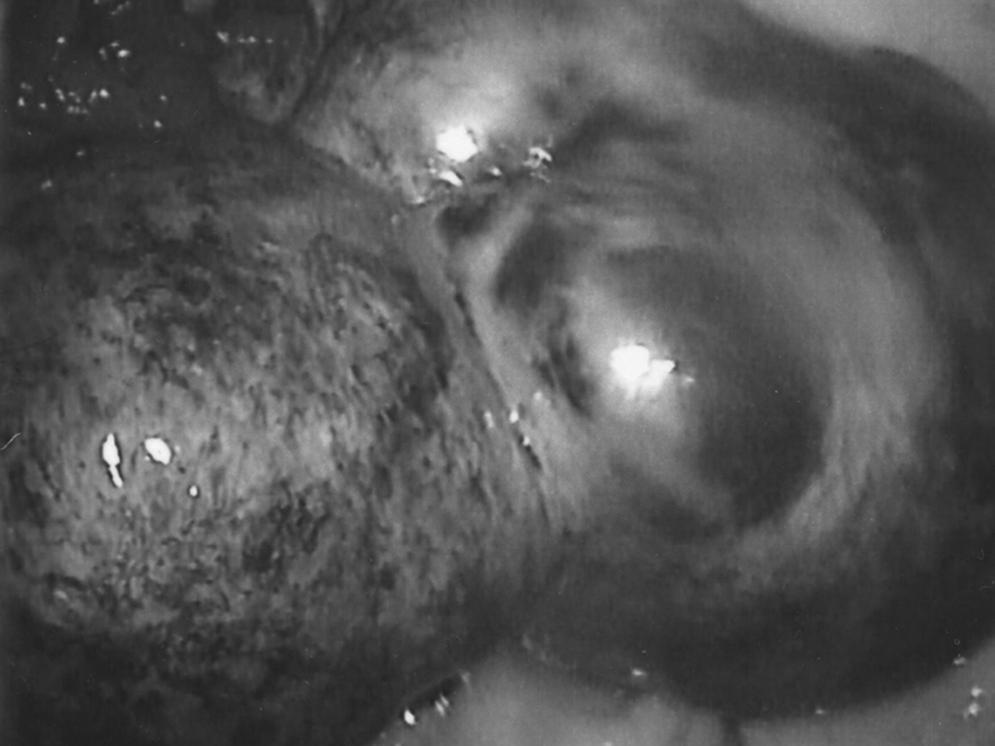
Bluish discoloration of an enlarged hyperstimulated ovary as a result of torsion. The change in tissue color is secondary to complete interruption of the blood supply.
The purpose of this article is to describe an unusual case of adnexal torsion that presented with acute abdominal pain in the absence of interruption of blood flow to the ovary on transvaginal ultrasound (US) Doppler flow study.
Case
A 32-year-old gravida 0, para 0 Caucasian female with a history of right unicornuate uterus and endometriosis presented for fertility treatment at IVF Michigan, PC after five failed cycles of in vitro fertilization and embryo transfer (IVF-ET) at another unit. The patient underwent two IVF cycles using intracytoplasmic sperm injection (ICSI) and ET. Both cycles resulted in pregnancy, but unfortunately, both pregnancies ended in miscarriage. During the third cycle, the patient underwent ICSI and tubal ET, which resulted in a viable twin pregnancy. She developed a mild form of ovarian hyperstimulation syndrome (OHSS). The diagnosis was made on transvaginal US scan, which showed both ovaries to be enlarged with multiple corpora lutea cysts, but no evidence of ascites. The right ovary measured 80 mm by 60 mm, whereras the left ovary measured 60 mm by 50 mm. This required observation on an outpatient basis. The patient presented to an emergency room with acute abdominal pain at ten weeks of gestation at 2:00 p.m., where the diagnosis of adnexal torsion was ruled out by transvaginal US Doppler flow study. The patient was given IV pain medications every 3 hours for pain relief, without any improvement in her symptoms. The possibility of hetero-ectopic pregnancy with one pregnancy being intrauterine and the other being a cornual ectopic pregnancy about to rupture was entertained. The patient was eventually transferred to our care at a local hospital via ambulance. Upon arrival 11 hours after the onset of her symptoms, an immediate laparoscopy was performed.
On laparoscopy, right adnexal torsion with two twists was documented in the absence of any change in color of the adnexa (Fig. 2), suggesting that torsion was enough to cause ischemic pain, but not complete interruption of blood flow. An enlarged pregnant unicornuate uterus at 10 weeks of gestation was seen without evidence of cornual pregnancy (Fig. 2). Both ovaries were enlarged (the right ovary was larger than the left ovary) with multiple corpora lutea cysts as a result of controlled ovarian stimulation and the effect of human chorionic gonadotropin with pregnancy. There was no evidence of any ascites, and in turn, no evidence of a severe form of OHSS. The enlarged right ovary, as a result of controlled ovarian stimulation, predisposed the patient to adnexal torsion.
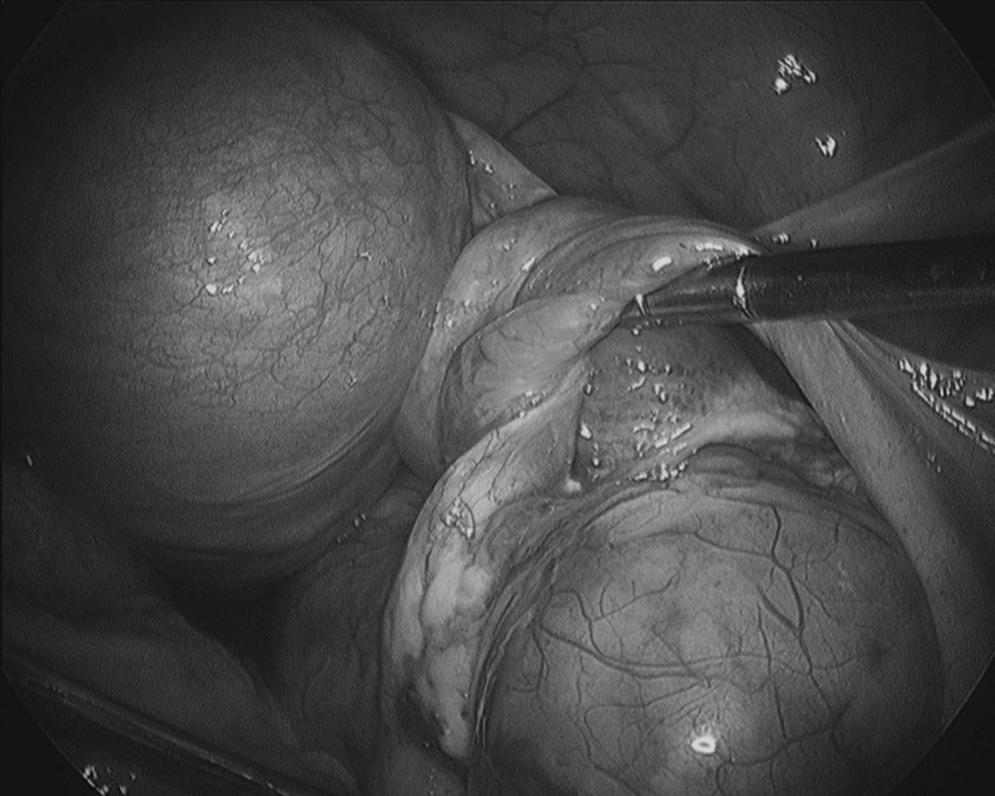
Enlarged unicornuate uterus as a result of pregnancy and right adnexal torsion with two twists, with no change in tissue color to suggest complete interruption of the blood supply.
Laparoscopic lifting of the ovary and untwisting of adnexa was performed (Figs. 3 and 4) followed by aspiration of ovarian cysts to decompress the ovary in an attempt to prevent recurring of torsion. The patient had an uneventful recovery and subsequently she delivered at 32 weeks of gestation. The newborns' birth weights were 1.56 kg and 1.43 kg respectively.

Laparoscopic lifting of the ovary and the start of untwisting of the adnexa.
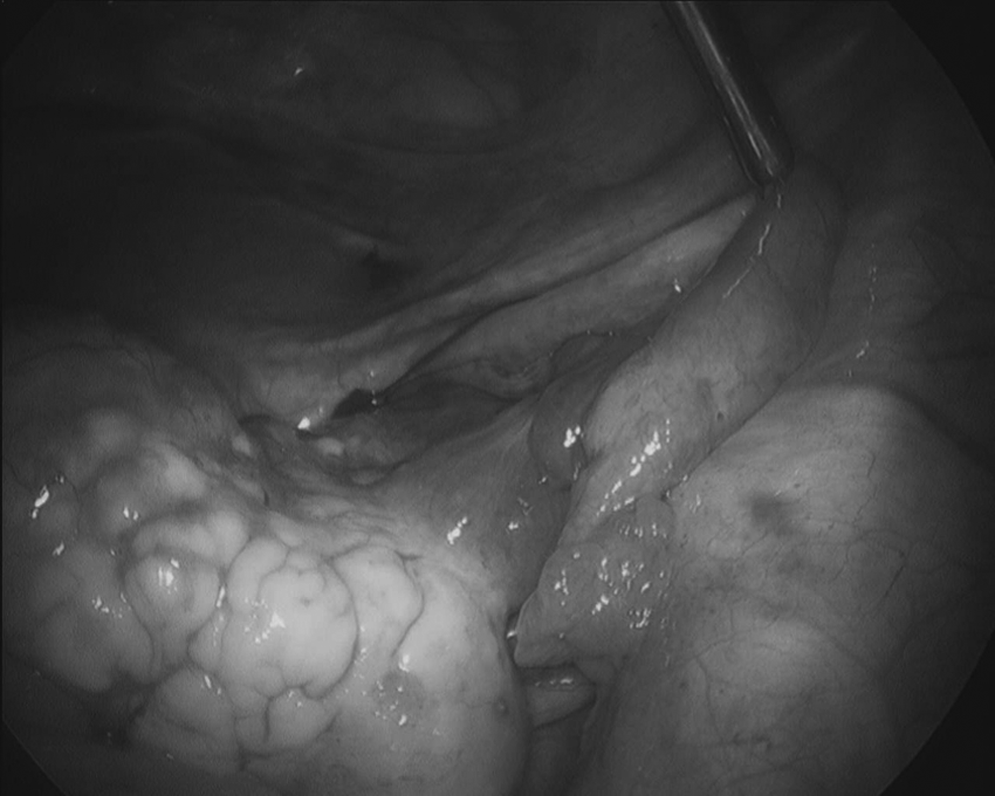
The right ovary and tube after untwisting of the adnexa.
Discussion
Several risk factors may have predisposed this patient to adnexal torsion. Such factors include enlarged ovaries after COS, pregnancy, twin pregnancy with higher human chorionic gonadotropin levels (which maintain ovarian enlargement), and, perhaps, the presence of a unicornuate uterus.
Patients presenting with adnexal torsion usually complain of an acute, intermittent, unilateral pelvic pain. Seventy percent of patients have associated gastrointestinal complaints such as nausea and vomiting. On physical examination, a tender, unilateral adnexal mass is appreciated in some patients. On abdominal examination, signs of acute abdomen are usually present. Diagnosis is often made by ruling out other causes and by having a strong clinical suspicion. A transvaginal US with color Doppler flow study illustrates interruption of blood flow to the ovary. 4 The diagnosis is confirmed and treatment of adnexal torsion is undertaken at the time of laparoscopy. The treatment of adnexal torsion is surgical detorsion of the adnexa. Laparoscopic evaluation should be performed followed by gentle untwisting of the adnexa followed by careful observation for up to 20–30 minutes to ensure viability of the adnexal tissue. Treatment should then be directed toward the underlying etiology. Ovarian cystectomy should be performed in the presence of a benign ovarian cyst. Alternatively, one should aspirate an enlarged cyst in the pregnant patient or multiple cysts after COS to help in preventing the recurrence of torsion. In a pregnant patient, as in this case, care should be taken to avoid touching the uterus during surgical manipulation, to reduce the risk of miscarriage. However, the pregnant patient should be counseled regarding the potential risks, including miscarriage, premature labor, preterm rupture of membranes, and preterm delivery. In cases of severe vascular compromise resulting in tissue necrosis, unilateral salpingo-oophorectomy should be performed.
This case report suggests that in patients presenting with acute abdomen with clinical manifestations of adnexal torsion, a normal transvaginal US Doppler flow should not exclude the possibility of adnexal torsion. In such cases, diagnostic laparoscopy is indicated to rule out adnexal torsion before tissue necrosis occurs, resulting in loss of the ovary. A recent similar case study showed a viable fallopian tube despite twisting twice along its blood supply. 5
Conclusions
The diagnosis of adnexal torsion should be suspected by the clinical presentation. Although a transvaginal US with color Doppler study can be highly predictive of adnexal torsion, a normal Doppler flow cannot rule out adnexal torsion resulting in ischemic changes without complete interruption of blood flow, as illustrated in this case. Diagnostic laparoscopy is the gold standard for the diagnosis and management of adnexal torsion.
Footnotes
Acknowledgment
The authors thank Cheryl Anderson for preparation of the manuscript.
Disclosure Statement
No competing financial conflicts exist.