
Abstract
Abstract
Introduction
H
Case
A 50-year-old Caucasian female, gravida 5, para 2, with two early spontaneous miscarriages, one ruptured ectopic pregnancy, and a low transverse CS with a diagnosis of secondary infertility presented to the authors' unit in 2005 requesting to undergo a second cycle of in vitro fertilization and embryo transfer (IVF-ET) using a donor egg program with her current husband.
Four years earlier, she had undergone a successful IVF-ET using a donor egg program that resulted in a singleton term pregnancy delivered by a primary low transverse CS. Three embryos were transferred into the uterine cavity under US guidance, and a pregnancy test was positive 2 weeks later. Transvaginal US examination at approximately 6 weeks' gestation revealed multiple gestation with a twin IUP and a third gestational sac implanted at the anterior wall of the lower uterine segment, at the site of the previous CS scar (Figs. 1 and 2). All three embryos had cardiac activity. The distance between the edge of the gestational sac in the CS scar and the edge of the closer IUP gestational sac was approximately 35 mm (Fig. 1). A diagnosis of heterotopic pregnancy in a CS scar was made. The patient had no discomfort, and her pelvic examination was unremarkable. The finding was relayed to the patient and her husband. After extensive counseling about the condition, its risks and treatment options, a conservative management strategy was adopted because of the patient's strong desire to preserve the twin IUP. Under intravenous sedation and sterile condition, a 16-gauge needle was used to aspirate the contents of the gestational sac in the CS scar under transvaginal US scan guidance. The patient tolerated the procedure well.

Transvaginal ultrasound scan picture showing a viable twin intrauterine pregnancy (IUP) compatible with 6 weeks' gestation and a third ectopic gestational sac containing a viable embryo seen in the anterior wall of the lower uterine segment at the site of a previous cesarean section (CS) scar (large arrow). The distance between the edge of the gestational sac in the CS scar and the edge of the closer IUP gestational sac was approximately 35 mm (small arrow).
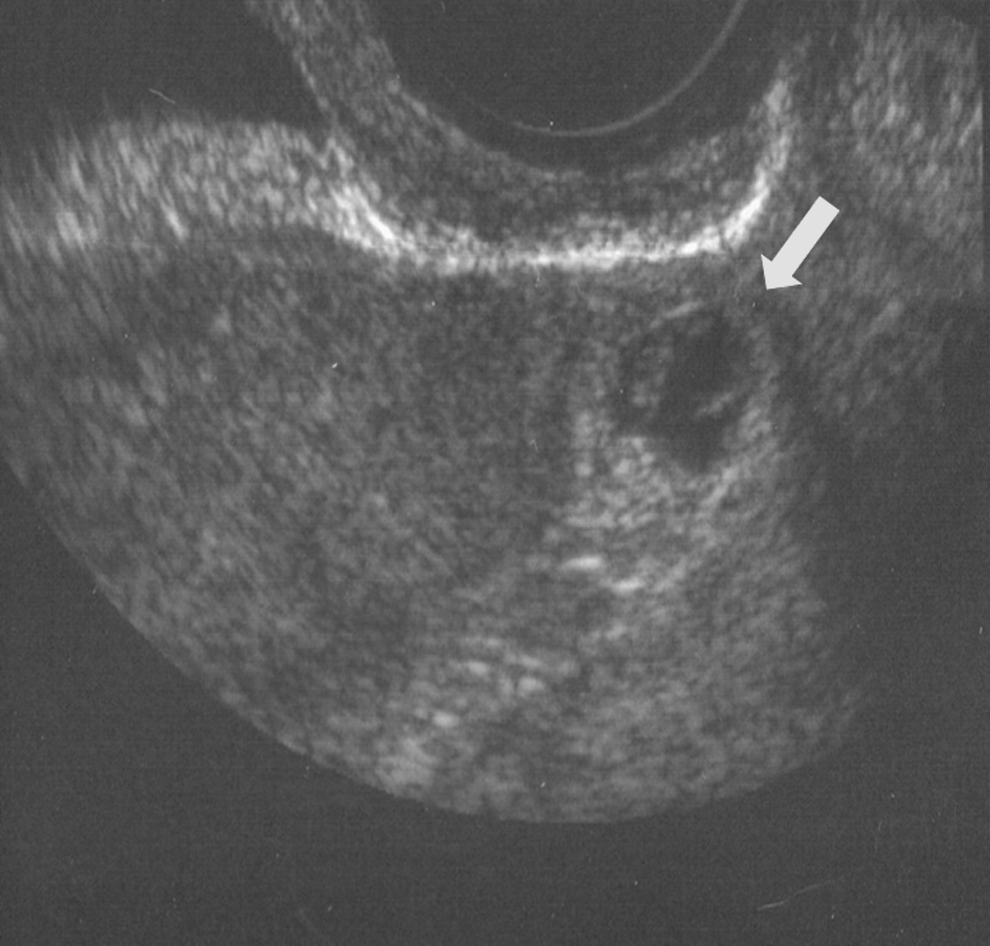
Transvaginal ultrasound scan of an ectopic gestational sac containing a viable embryo located in the anterior wall of the lower uterine segment at the site of a previous cesarean section scar (arrow).
After 1 week, a repeat US showed a viable twin IUP and the persistence of a CS gestational sac, but no evidence of fetal pole or cardiac pulsations was seen at that time (Fig. 3). It was explained to the patient that trophoblastic tissue can be active in the absence of an embryo and, in turn, she was still at risk for possible complications. Transvaginal US was repeated 5 days later with the same findings reported in the previous examination, with no increase in size of the ectopic gestational sac and a normal viable twin IUP at 8-week gestation. Four weeks later, another transvaginal US scan was performed, which revealed shrinkage and almost complete resorption of the gestational sac (Fig. 4). The twin IUP proceeded without further complications until 32-week gestation, when a repeat low transverse CS was performed because she had developed preeclampsia. At the time of her CS, there was no evidence of dehiscence at the site of the cesarean scar. Following the delivery, the low transverse CS incision in the uterus was sutured using 0-Vicryl in two layers in continuous running manner.

Transvaginal ultrasound scan (US) scan of a repeat US scan showing a viable twin intrauterine pregnancy at 7 weeks' gestation and the persistence of cesarean section gestational sac, but no evidence of fetal pole (arrow).

Transvaginal ultrasound scan showing shrinkage and almost complete resorption of ectopic gestational sac in the cesarean section scar and a viable twin intrauterine pregnancy at 11 weeks' gestation.
Discussion
Ectopic pregnancy in a CS scar (CSP) is the implantation of a pregnancy within a cesarean fibrous tissue scar. It is the most rare form of ectopic pregnancies. The diagnosis and treatment have changed dramatically in the last 20 years. Before 1980, CSP would often present with life-threatening hemorrhage and uterine rupture requiring emergency hysterectomy. Now, it is commonly diagnosed on a first trimester US. The number of cases described in the literature appear to be much higher since 2002, presumably because of an increase in the number of cesarean procedures currently being performed, as well as the more widespread use of transvaginal US that enable an earlier detection of such pregnancies. The sonographic criterion for the diagnosis of CSP is the presence of gestational sac in the anterior part of the isthmic portion of the uterus. Occasionally CSP can be visualized in between the bladder and the gestational sac. Other diagnostic tools such as magnetic resonance imaging, cystoscopy, hysteroscopy, and laparoscopy can also be used.
Two possible conservative treatment options may be considered: medical or surgical. Both aim to eliminate the gestational sac and preserve the patient's fertility. Medical treatment with systemic or local injection of methotrexate (MTX) has been reported. Recently, Nawroth et al. also described the combined effect of local and systemic MTX administration with or without aspiration. 6 Potassium chloride (KCL), or hyperosmolar glucose, or a hypertonic solution of sodium chloride has been used as well.3,7,8 Heterotopic pregnancy is the coexistence of IUP and extrauterine pregnancy. Its incidence has increased with the widespread use of assisted reproductive technology (ART). The diagnosis can be difficult; heterotopic pregnancies often escape early recognition because both serum β-human chorionic gonadotropin and US can be misleading, and the diagnosis is not made until ectopic rupture with internal hemorrhage and shock. Gupta et al. reported a ruptured ectopic pregnancy in a CS scar at 9-week gestation necessitating laparotomy and hysterectomy. 9 They concluded that early diagnosis is very important to avoid catastrophic hemorrhage and to avoid the need for surgery. 9 The current authors believe that the successful outcome in the case described in this article can be attributed to early diagnosis and management.
Heterotopic CSP is extremely rare, and its occurrence in conjunction with a viable IUP and the patient's desire to keep the IUP make management very challenging. Salomon et al. described a heterotopic CSP with one embryo implanted into the uterine cavity, and the other located in the anterior isthmus wall that was successfully managed with KCL injection into the embryo to terminate the CSP at 8 weeks of gestation. 10 Other reports have shown that during the injection of KCL, the embryo is sometimes pushed away from the needle and KCL diffuses into the amniotic sac. Consequently, it may diffuse to the adjacent sac and cause a toxic effect on the remaining embryo(s). A surgical option with laparotomy and excision of the cesarean ectopic from the lower uterine segment and repair was also proposed. 11 The patient in the present report did not want to take any chance and emphasized the need for preserving the intrauterine twin pregnancy; therefore, the authors opted for the most conservative management possible.
To the authors' knowledge, the current case is the third reported heterotopic CSP, and the second to be successfully treated with US-guided aspiration. Hsieh et al. (2004) reported a similar case that was successfully treated with US-guided aspiration, and twin IUP was successfully preserved to be delivered at 32 weeks of gestation because of preterm labor. 12
Conclusions
In view of the increasing number of CS being performed and the use of ART, obstetricians should be aware of the possibility of this type of heterotopic pregnancy. The present reinforces what was reported by Hsieh and suggests that a heterotopic CS ectopic pregnancy can be successfully treated with US-guided aspiration if diagnosis is made early in pregnancy.
Footnotes
Acknowledgments
The authors wish to thank Cheryl Anderson for preparation of the manuscript.
Disclosure Statement
The authors have no commercial, proprietary, or financial interest in the products or companies described in this article.