
Abstract
Abstract
Introduction
Case
A 36-year-old-woman presented with primary infertility of 2 years duration. Her associated complaints were menorrhagia and known uterine fibroids. She underwent a hysteroscopic myomectomy 2 years earlier without any relief in her symptoms. An hysterosalpingogram revealed that the uterine cavity was occupied and compromised by a large, smooth, filling defect, most probably representing a submucous fibroid (Fig. 1). Transvaginal 2D ultrasound with a saline infusion hysterosonogram (SIH) showed an 8-cm large anterior-fundal submucous intramural fibroid reaching and stretching the serosal layer (type II submucous fibroid; Fig. 2). A diagnostic hysteroscopy and laparoscopy confirmed the ultrasound findings. The myoma was injected at its base with 20 cc of diluted vasopressin (20 units in 100 cc of normal saline). A transverse incision was made over the uterine serosa onto the surface of the myoma using a laparoscopic spatula with monopolar cautery (40 W cutting current), and the incision was extended until the capsule of the myoma was reached. The capsule was opened and the myoma was enucleated using a single-toothed myoma grasper. The capsule was then dislocated from the uterine bed and the laparoscopic myomectomy was completed (Fig. 3). After dissecting the myoma, it was noted that the endometrial cavity was entered in a small area (about 1 cm), and there was moderate amount of bleeding from the myometrium (Fig. 4). Therefore, laparoscopic repair was deemed inappropriate. A minilaparotomy was performed to repair the endometrial cavity and overlying myometrium adequately. A 5-cm transverse skin incision was made in the suprapubic region, and the skin was dissected in an upward and downward fashion to allow us to make a longitudinal incision in the fascia (Fig. 5). The rectus muscles were separated in the midline, and the peritoneum cavity was entered in a routine fashion. The uterus was lifted up partially through the minilaparotomy incision using a uterine manipulator to facilitate suturing. This allowed us to visualize the myometrial defect, which was repaired in three layers. The myoma was easily and rapidly morcellated using a scalpel. A pediatric Foley catheter (10 French) was placed into the uterine cavity, and its balloon was inflated with 5 cc of normal saline to reduce intrauterine scar-tissue formation. The patient was admitted for observation for 23 hours. Her postoperative course was uneventful. She was instructed to increase her activity gradually during the first 10 days following surgery. The patient was able to go back to work and resume regular activity after 3 weeks. The catheter was removed after 6 days. The patient was given high-dose estrogen (Estrace 2 mg bid; Ferring Pharmaceuticals, Inc., Parsippany, NJ) for 6 weeks with progestogen (Provera, 10 mg q d; Pfizer, Inc. New York City, NY) for the last 10 days. An SIH that was done 7 weeks postoperatively revealed a uniform endometrial cavity with no filling defects or synechiae.
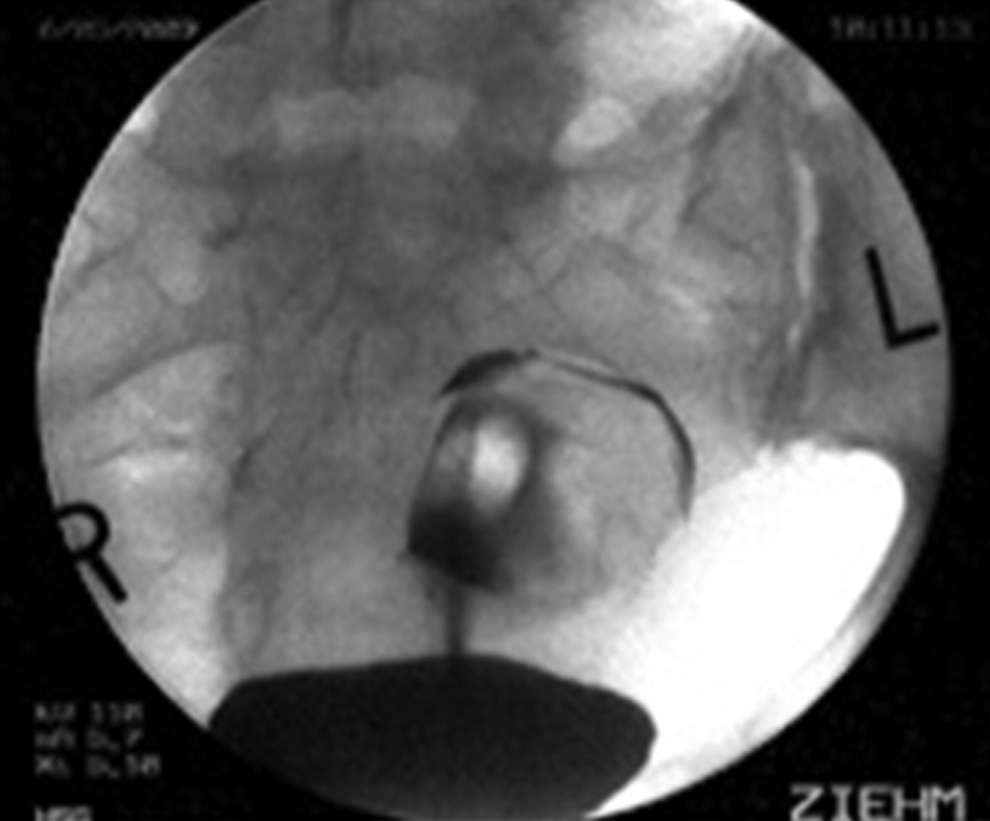
Hysterosalpingogram picture showing the uterine cavity to be occupied and compromised by a large filling defect with a smooth surface, most probably representing a submucous myoma. Taken from ISBN: HB 9781107029743. Edited by Botros R.M.B. Rizk and Elizabeth Puscheck. Ultrasonography in Gynecology. Figure 14 in the book chapter “Transvaginal ultrasound scan findings of uterine fibroid effect on treatment plan.” By Dr. Mostafa Abuzeid and Salem Joseph. Copyright © 2012 Cambridge University Press. Reprinted with the permission of Cambridge University Press.
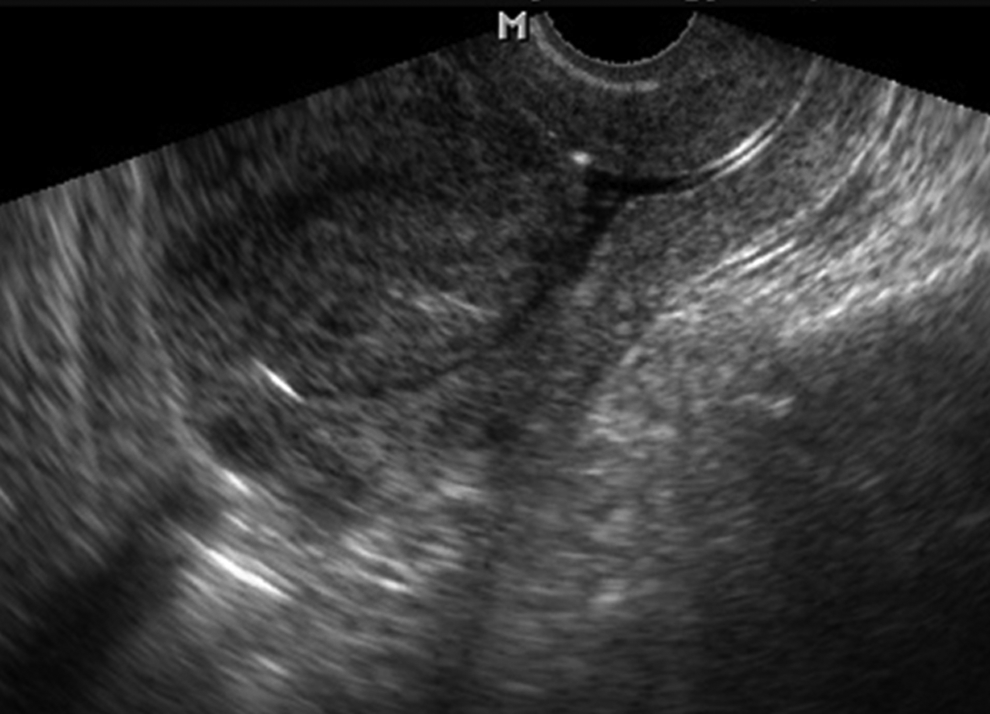
Transvaginal 2D ultrasound with saline infusion hysterosonogram picture showing an 8-cm large anterior-fundal submucous intramural fibroid reaching and stretching the serosal layer (type 2 submucous fibroid). Taken from ISBN: HB 9781107029743. Edited by Botros R.M.B. Rizk and Elizabeth Puscheck. Ultrasonography in Gynecology. Figure 15 in the book chapter “Transvaginal ultrasound scan findings of uterine fibroid effect on treatment plan.” By Dr. Mostafa Abuzeid and Salem Joseph. Copyright © 2012 Cambridge University Press. Reprinted with the permission of Cambridge University Press.
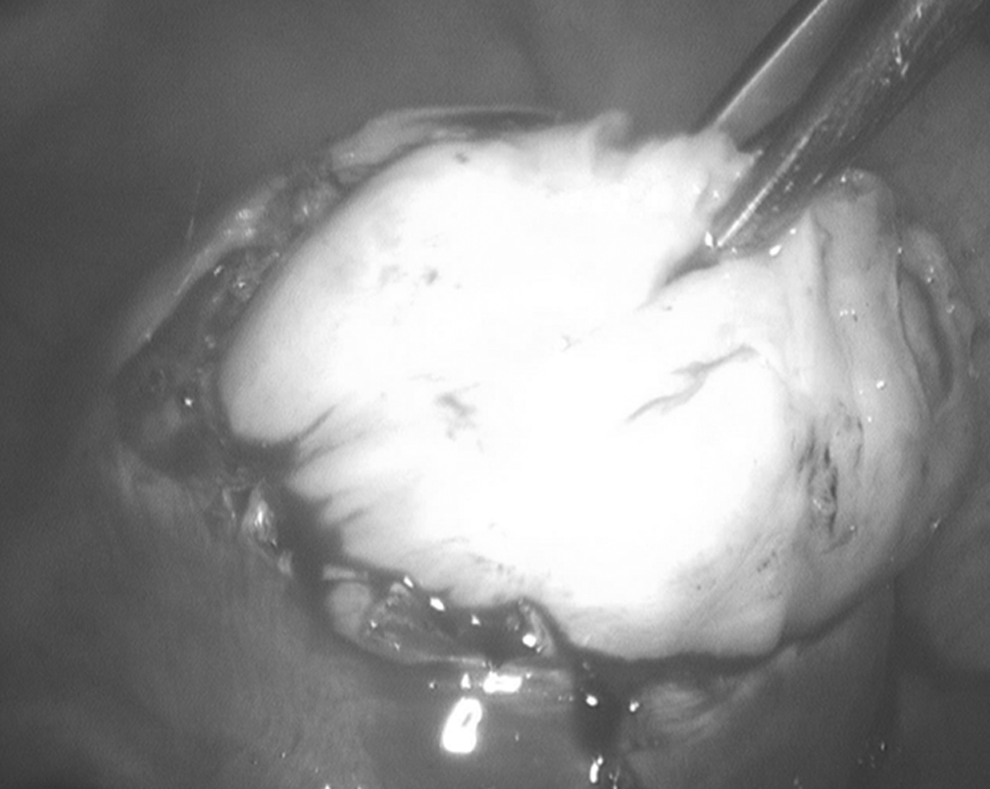
Laparoscopic picture depicting the dissection of the myoma. Taken from ISBN: HB 9781107029743. Edited by Botros R.M.B. Rizk and Elizabeth Puscheck. Ultrasonography in Gynecology. Figure 16 in the book chapter “Transvaginal ultrasound scan findings of uterine fibroid effect on treatment plan.” By Dr. Mostafa Abuzeid and Salem Joseph. Copyright © 2012 Cambridge University Press. Reprinted with the permission of Cambridge University Press.
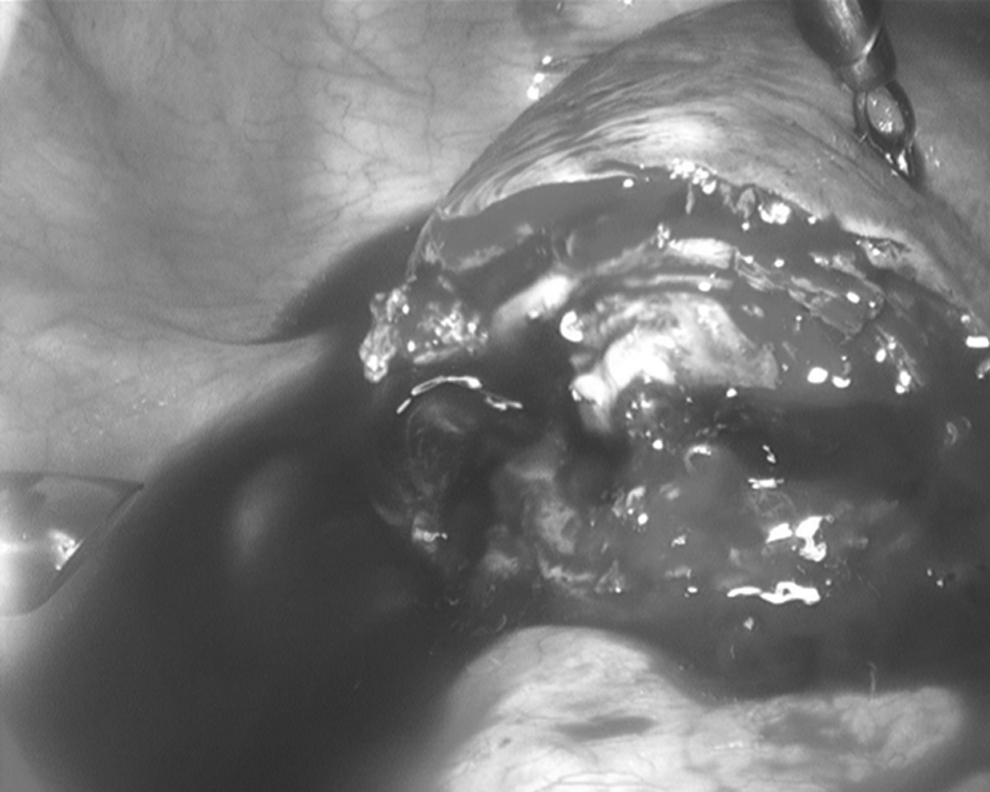
Laparoscopic picture depicting the myoma bed. Notice that the endometrial cavity was entered in a small area (about 1 cm) and a moderate amount of bleeding from the myometrium was observed. Taken from ISBN: HB 9781107029743. Edited by Botros R.M.B. Rizk and Elizabeth Puscheck. Ultrasonography in Gynecology. Figure 17 in the book chapter “Transvaginal ultrasound scan findings of uterine fibroid effect on treatment plan.” By Dr. Mostafa Abuzeid and Salem Joseph. Copyright © 2012 Cambridge University Press. Reprinted with the permission of Cambridge University Press.

A postoperative picture showing a 5-cm transverse suprapubic scar from the minilaparotomy. Taken from ISBN: HB 9781107029743. Edited by Botros R.M.B. Rizk and Elizabeth Puscheck. Ultrasonography in Gynecology. Figure 18 in the book chapter “Transvaginal ultrasound scan findings of uterine fibroid effect on treatment plan.” By Dr. Mostafa Abuzeid and Salem Joseph. Copyright © 2012 Cambridge University Press. Reprinted with the permission of Cambridge University Press.
Results
Five months later, the patient conceived spontaneously. Unfortunately, this pregnancy was terminated at 20 weeks gestation because of trisomy 18.
Discussion
We believe that an hysteroscopic myomectomy was not an option in our case because of the size and location of the fibroid. In fact, it was tried once on our patient at another hospital without any significant reduction in the size of the fibroid tumor. Traditionally, a large type II submucous fibroid is dealt with via laparotomy and myomectomy. Robotic-assisted laparoscopic myomectomy can now be used successfully to treat such cases. However, the da Vinci Surgical System is not available in many counties, and the cost associated with the procedure can be prohibitive. In addition, the introduction of V-Loc™ sutures (Covidian, Mansfield, MA) may allow experienced endoscopic surgeons to repair the myometrial defect seen in our patient adequately and safely.
The technique described in this case of laparoscopic myomectomy with minilaparotomy to rapidly morcellate the tumor and repair the myometrial defect is an alternative, safe, and effective approach of minimally invasive surgery for such patients. This technique can also be utilized by gynecologists with limited laparoscopic suturing skills. The technique has been described by our group, 8 and other authors have also described similar techniques of laparoscopic myomectomy and minilaparotomy as an alternative minimally invasive approach for the treatment of uterine fibroids.9–11 However, strong consideration should be given to referring such patients to another surgeon with the laparoscopic skills required to close the uterus laparoscopically if available.
Conclusions
The technique of minimally invasive surgery for the treatment of large type II submucous uterine fibroids described in this case can be performed successfully by a gynecologist with adequate laparoscopic training but limited laparoscopic suturing abilities. It is safe, effective, and avoids the need for traditional laparotomy in most cases of uterine fibroids without the expense associated with robotic-assisted myomectomy. However, such patients may need to be referred to another surgeon with advanced laparoscopic skills that might be needed to complete the procedure.
Footnotes
Acknowledgments
The authors would like to thank Cheryl Anderson for preparation of this manuscript. This paper was presented at the 39th Global Congress of Minimally Invasive Gynecology (AAGL), Las Vegas, Nevada, November 8–12, 2010 poster; Abstract #683, J Min Invas Gynecol 2010;17:S156.
Disclosure Statement
No competing financial interests exist.