
Abstract
Abstract
Introduction
Case
The patient discussed in this report was a 39-year-old Asian female who presented to the infertility clinic for evaluation of primary infertility of 9 years' duration. Her past medical history was remarkable for adult-onset diabetes mellitus since 2003, which was well-controlled with insulin and metformin. At age 35, a hysterosalpingogram (HSG) as part of an evaluation for her infertility at a different infertility clinic suggested that she had a T-shaped uterus and patent fallopian tubes. However, a subsequent diagnostic hysteroscopy suggested that she had a normal endometrial cavity. This patient had irregular periods and was diagnosed with polycystic ovarian syndrome (PCOS), for which she was treated with clomiphene citrate for five cycles without success. She had undergone one cycle of in-vitro fertilization with embryo transfer (IVF/ET) but was unable to conceive.
In view of the multiple infertility factors, which included her advanced female reproductive age and her long-term duration of infertility, this patient was offered IVF-ET treatment. A saline sonohysterogram with both two-dimensional (2D) and three-dimensional (3D) ultrasound (US) were performed prior to the IVF treatment. The 3D US suggested that she had a T-shaped uterus. IVF-ET was then performed; unfortunately, the patient did not conceive. At that stage, the patient was offered a review hysteroscopy to evaluate her endometrial cavity before any further attempts at IVF-ET. A diagnostic hysteroscopy revealed an arcuate appearance of the fundal region (Fig. 1) and a T–shaped cavity. Using a straight monopolar resectoscope loop with a cutting current of 70 Watts, division of the short uterine septum in the fundal region was performed. Care was taken to work at equal distance from both the anterior and posterior walls. After cutting through the first part in the middle of the segment, a hole was noticed (Fig. 2), and some turbid fluid was seen coming from an area above the hole. This hole had a cavity above it leading to the uterine fundus. The next step was to incise what was thought to be a thin membrane that was transversely stretched between the two uterine cornua. Upon completing this step the uterine fundus became visible and this revealed an arcuate uterus. The short uterine septum was divided easily, using a straight monopolar resectoscope loop with a cutting current of 70 Watts, without any problems (Fig. 3). The T-shaped cavity was confirmed (Fig. 4), and hysteroscopic metroplasty was performed by incising the lateral uterine-wall ridges, using a monopolar resectoscope loop with a curved needle tip and using a cutting current of 70 Watts. Upon completing the procedure both tubal ostia became visible. Hemostasis was ensured. At the end of the procedure, a pediatric Foley catheter (8 French) was introduced into the uterine cavity and the catheter balloon was inflated with 3 cc of normal saline. The catheter was removed after 10 days. The patient was placed on exogenous estrogen for 6 weeks followed by progestin for 10 days.

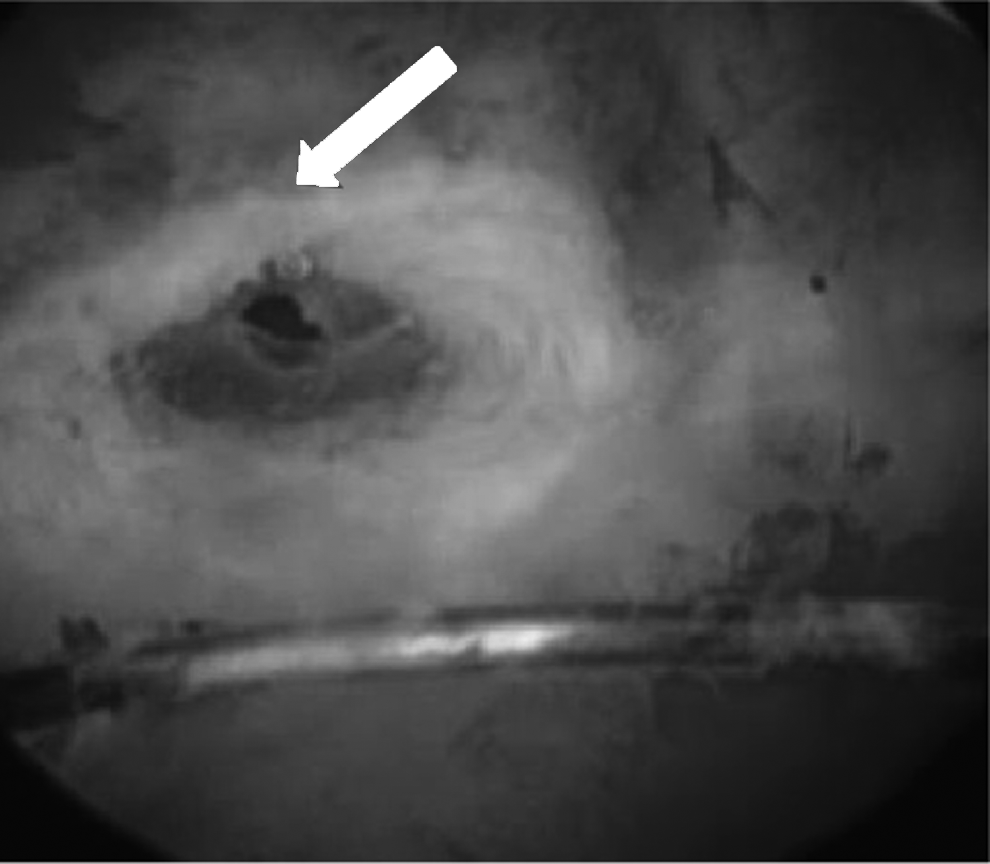
Hysteroscopic picture depicting an arcuate appearance of the fundal region of the uterus (arrow) before the start of the surgical procedure.
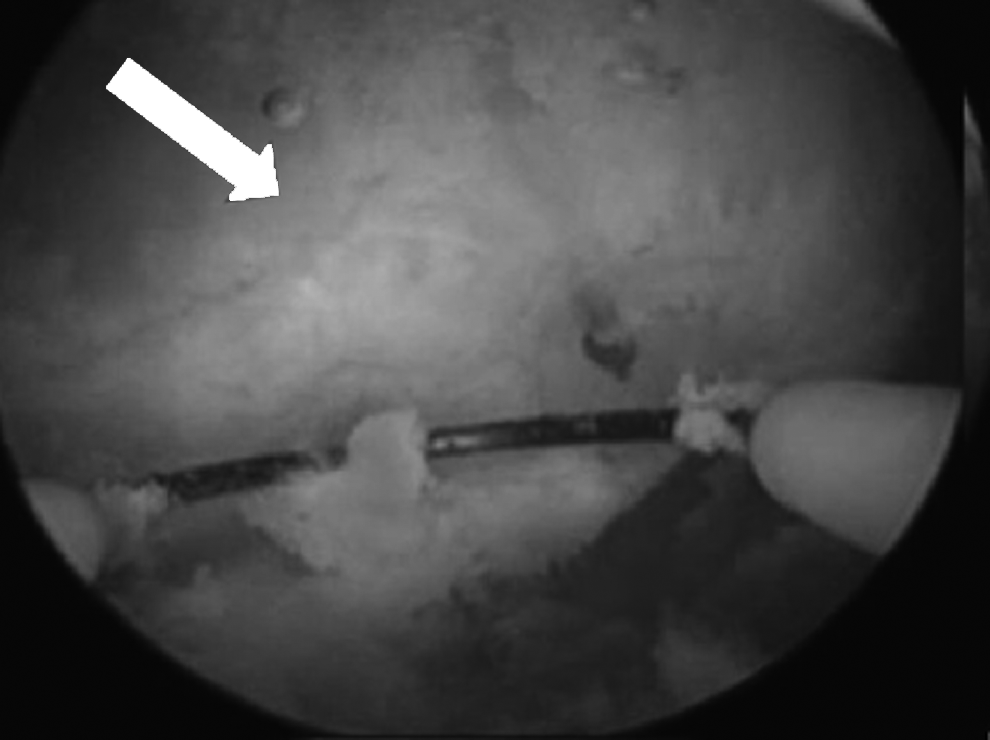
Hysteroscopic picture depicting a hole in a trans-fundal membrane (arrow) that was obscuring the uterine fundus.
Hysteroscopic picture depicting the fundus of the uterine cavity (arrow) after the trans-fundal membrane was incised and the arcuate fundus was divided.
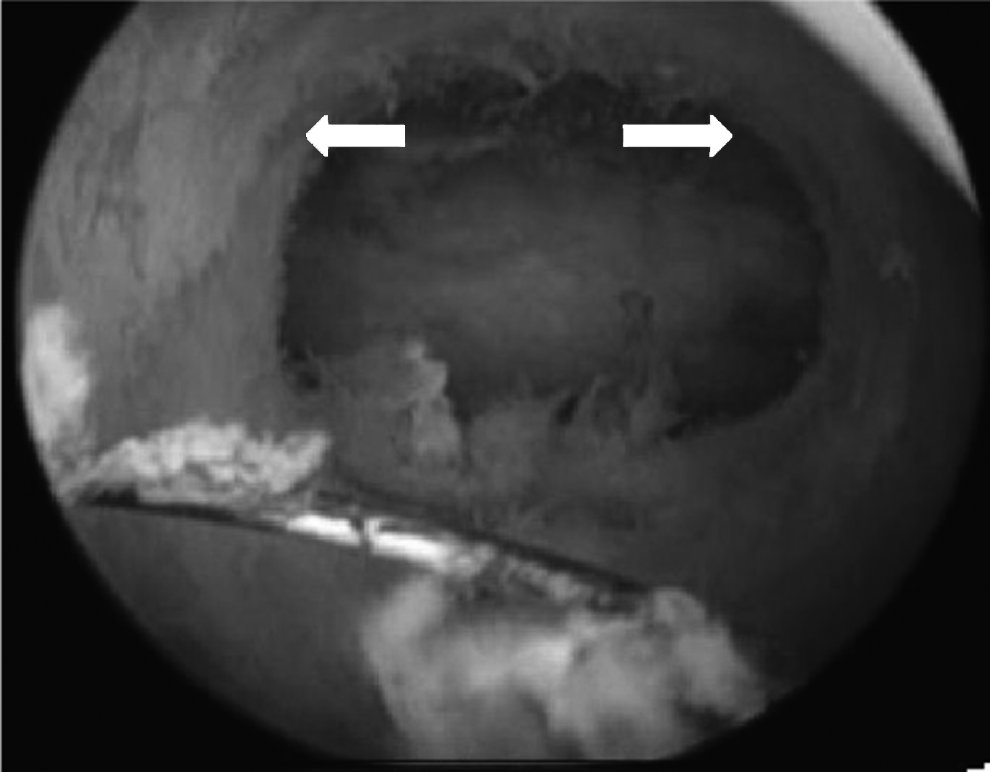
Hysteroscopic picture with arrows pointing toward the lateral walls of a T-shaped cavity before hysteroscopic surgical correction of the lateral walls.
Results
Subsequently, saline sonohysterograms (both 2D and 3D US) revealed a normal endometrial cavity. The postoperative period was uneventful. Three months later, IVF/ET was attempted. The patient conceived but had an early miscarriage. Following a second IVF/ET cycle, the patient conceived and delivered a healthy male infant at full-term.
Discussion
Patients with uterine anomalies have increased chances of spontaneous and recurrent miscarriages, intrauterine growth restriction (IUGR), preterm labor, preterm delivery, and infertility.2,6–8 Uterine septum and arcuate uterus are the most common uterine anomalies, accounting for 34% and 33%, respectively.5,9 Therefore, a comprehensive evaluation of the endometrial cavity is important to identify any abnormalities that may affect reproductive outcomes. 4 The goal of management is to achieve a normal uterine architecture if the uterine anomaly can be repaired (e.g., uterine septum and arcuate uterus). Over the last 3 decades, hysteroscopic division of the uterine septum has replaced the transabdominal approach and has been shown to be safe and effective, as well as significantly improving subsequent reproductive outcomes. 10
Controversy still exists regarding the management of patients with T-shaped uteri. Many reproductive surgeons advocate no treatment, citing the fact that some patients with T-shaped uteri have favorable reproductive outcomes. However, over the past 2 decades, hysteroscopic metroplasty for T-shaped uteri has been advocated by some researchers with promising results. 11 The patient described in this case report had two failed IVF-ET cycles, and she was running out of time in view of her reproductive age. What complicated the management of this patient was the fact that she had a hysteroscopy that was reported to show normal results, despite the finding on her HSG. This point highlights an important issue regarding the interpretation of various diagnostic procedures, including the “gold standard” for diagnosis of uterine anomalies (i.e., diagnostic hysteroscopy).
The successful outcome of treatment of this patient was most probably secondary to correction of the T-shaped cavity, short uterine septum, and, most importantly, the discovery and correction of this subtle uterine pathology in the form of a trans-fundal uterine membrane. The current authors believe that this membrane was not a healthy site for embryo implantation.
Conclusions
Hysteroscopy by an experienced individual is a reliable diagnostic tool for evaluating uterine-cavity abnormalities. Hysteroscopic correction of subtle endometrial-cavity pathology reduces implantation failure and enhances chances for better reproductive outcomes.
Footnotes
Acknowledgments
The authors would like to thank Cheryl Anderson for the preparation of the manuscript.
Disclosure Statement
The authors, Reda Alami, MD, John Hebert, MD, Mohammad Ashraf, MD and Motafa Abuzeid, MD, have no commercial, proprietary, or financial interest in the products or companies described in this article.