
Abstract
Abstract
Introduction
Case
A 30-year-old white female presented with the chief complaint of recurrent miscarriages (on two occasions) at 10 weeks' gestation over a period of 2 years. She and her partner underwent complete work-up for recurrent pregnancy loss, including karyotype analysis on both husband and wife, complete thrombophilia testing, anticardiolipin antibodies, lupus anticoagulant antibody test, and TSH level. All laboratory tests were normal. On transvaginal ultrasound scan (US) and a saline infusion hysterosonogram (SIH) with both 2D and 3D US, the patient was found to have a 3×2 cm submucosal, intramural, subserosal fundal fibroid (Fig. 1). According to the European Society for Gynecological Endoscopy (ESGE), the fibroid in this patient was classified as a type II submucosal fibroid. 4 The fibroid was removed via laparoscopic myomectomy, and the myometrial defect was repaired in two layers using a continuous running 2-0 Vicryl suture (Figs. 2–4). The endometrial cavity was not entered. Hysteroscopy was performed at the conclusion of the procedure, which showed a possible concurrent incomplete short uterine septum with a wide base, rather flat apex, and mid-fundal length of about 1.5 cm versus a possible fundal indentation secondary to suturing of the myometrial defect status post myomectomy (Fig. 5). The other possibility was that the fundal filling defect was due to the distortion caused by suturing the myometrial defect. It was deemed appropriate that no further action should be taken at that time, since we were not sure of the diagnosis. In addition, even if an associated incomplete short uterine septum was present, it could not be corrected for fear of cutting the myomectomy sutures, risk of uterine perforation, and excessive bleeding. The patient was advised to return for a follow-up saline sonogram after healing from surgery to confirm the diagnosis of a uterine septum. The patient failed to attend for follow up, which led her to have three more miscarriages and one chemical pregnancy. This happened over a period of 18 months after removal of the fibroid. When the patient returned for follow up, an SIH was performed, which confirmed our earlier suspicion of an incomplete short uterine septum. A diagnostic hysteroscopy confirmed the diagnosis (Fig. 6a and b), and the patient underwent hysteroscopic division of the short uterine septum (Fig. 7). Dilatation and curettage was performed at the end of this procedure, and chronic endometritis was ruled out based on the pathology report of the endometrial curetting. Six weeks postoperatively, SIH showed a normal uterine cavity. The patient and her husband were treated with a course of doxycycline (Vibramycin) for 10 days starting with menses for treatment of any possible cervical infection that can lead to miscarriage such as mycoplasma genitalium. Premenstrual endometrial biopsy (EMB) was not performed in view of reports that questioned the accuracy of EMB in the diagnosis of luteal phase defect (LPD). 5 However, progesterone supplementation was planned 3 days after ovulation or with a positive pregnancy test for treatment of any possible LPD.

Transvaginal 3D ultrasound with saline infusion hysterosonogram showing a 3×2 cm submucosal intramural subserosal fundal fibroid (type II submucosal fibroid). Taken from ISBN: HB 9781107029743. Edited by Botros R.M.B. Rizk and Elizabeth Puscheck. Ultrasonography in Gynecology. Figure 1 in the book chapter “Transvaginal ultrasound scan findings of uterine fibroid effect on treatment plan.” By Dr. Mostafa Abuzeid and Salem Joseph. Copyright © 2012 Cambridge University Press. Reprinted with the permission of Cambridge University Press.
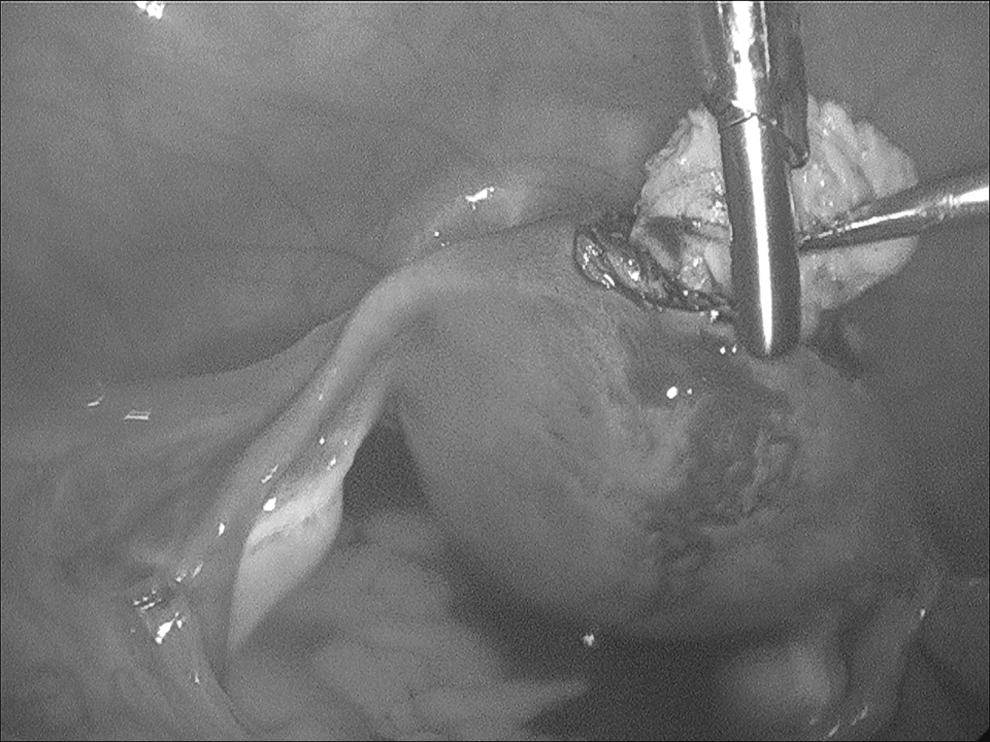
Laparoscopic picture showing dissection of a fundal uterine fibroid. Taken from ISBN: HB 9781107029743. Edited by Botros R.M.B. Rizk and Elizabeth Puscheck. Ultrasonography in Gynecology. Figure 2 in the book chapter “Transvaginal ultrasound scan findings of uterine fibroid effect on treatment plan.” By Dr. Mostafa Abuzeid and Salem Joseph. Copyright © 2012 Cambridge University Press. Reprinted with the permission of Cambridge University Press.
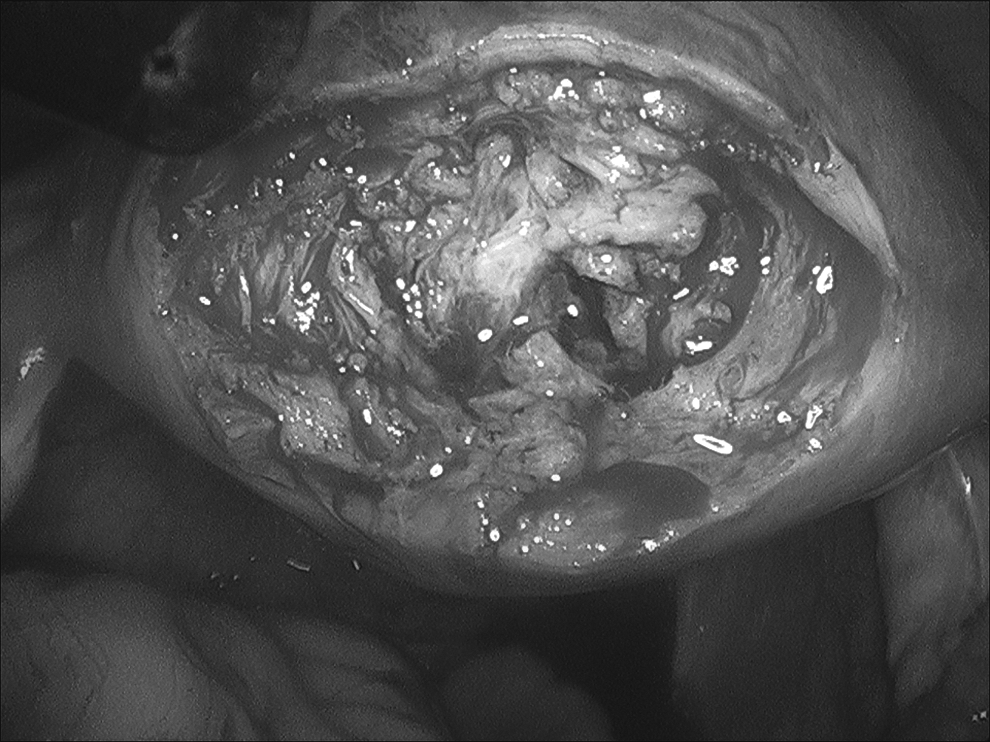
Laparoscopic picture showing the myometrial defect after removal of a fundal uterine fibroid. Taken from ISBN: HB 9781107029743. Edited by Botros R.M.B. Rizk and Elizabeth Puscheck. Ultrasonography in Gynecology. Figure 3 in the book chapter “Transvaginal ultrasound scan findings of uterine fibroid effect on treatment plan.” By Dr. Mostafa Abuzeid and Salem Joseph. Copyright © 2012 Cambridge University Press. Reprinted with the permission of Cambridge University Press.
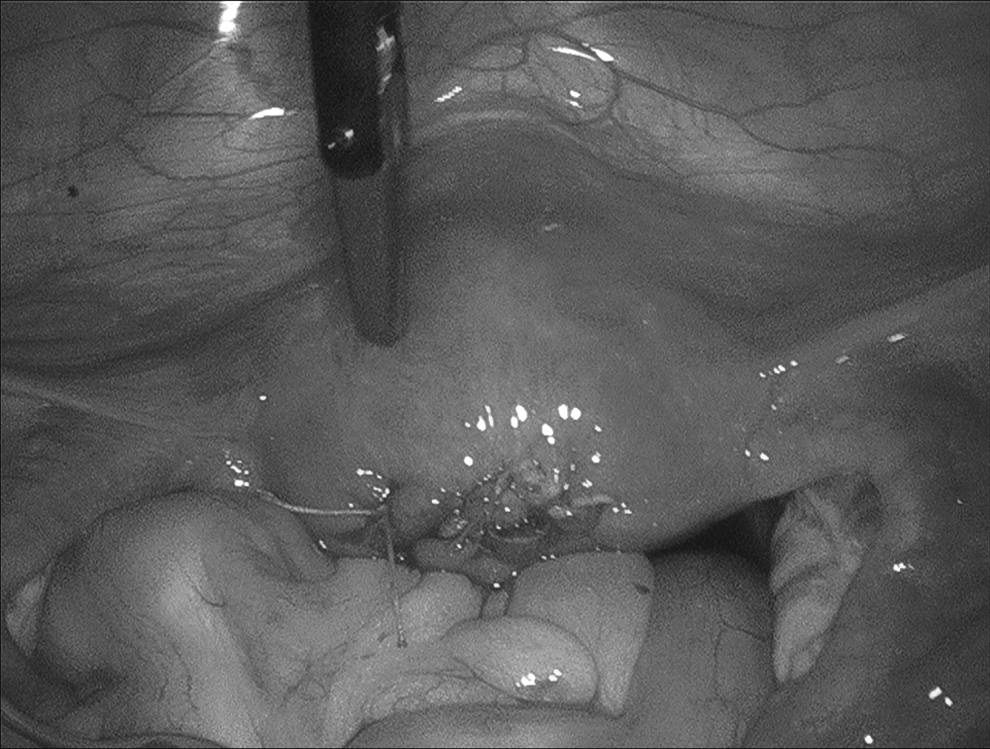
Laparoscopic picture showing the myometrial defect sutured in two layers. Taken from ISBN: HB 9781107029743. Edited by Botros R.M.B. Rizk and Elizabeth Puscheck. Ultrasonography in Gynecology. Figure 4 in the book chapter “Transvaginal ultrasound scan findings of uterine fibroid effect on treatment plan.” By Dr. Mostafa Abuzeid and Salem Joseph. Copyright © 2012 Cambridge University Press. Reprinted with the permission of Cambridge University Press.
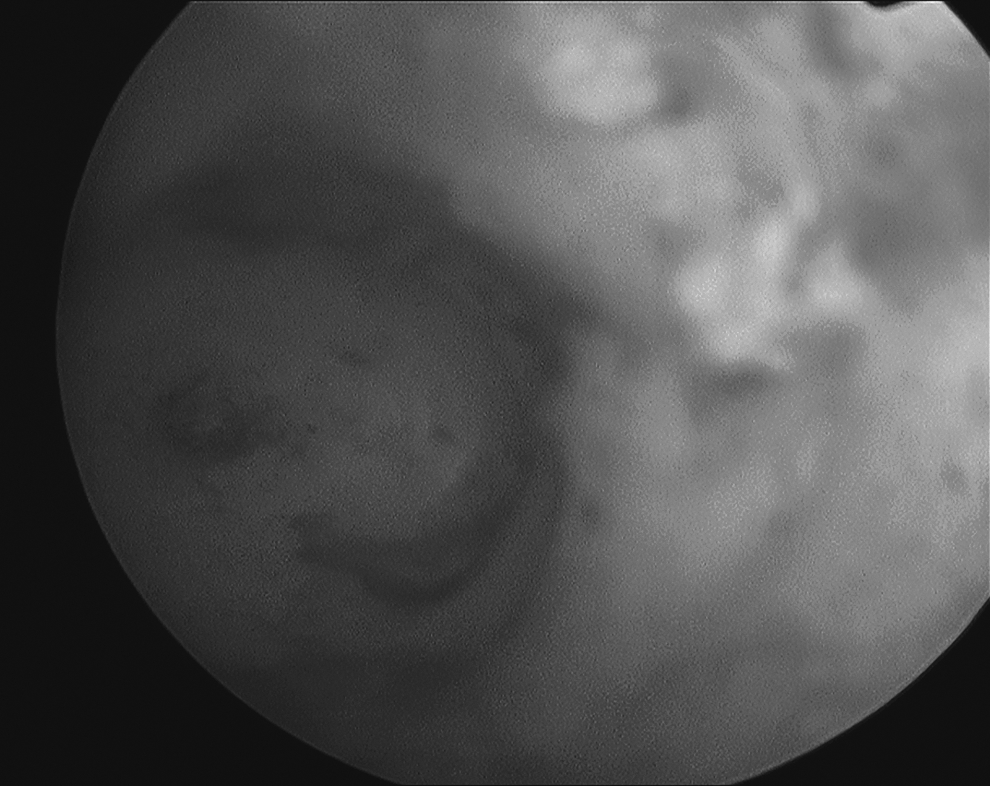
Hysteroscopic picture at the conclusion of the laparoscopic myomectomy showing the right cornual region with tubal ostium and right portion of a possible incomplete short uterine septum. Taken from ISBN: HB 9781107029743. Edited by Botros R. M. B. Rizk and Elizabeth Puscheck. Ultrasonography in Gynecology. Figure 5 in the book chapter “Transvaginal ultrasound scan findings of uterine fibroid effect on treatment plan.“ By Dr. Mostafa Abuzeid and Salem Joseph. Copyright © 2012 Cambridge University Press. Reprinted with the permission of Cambridge University Press.
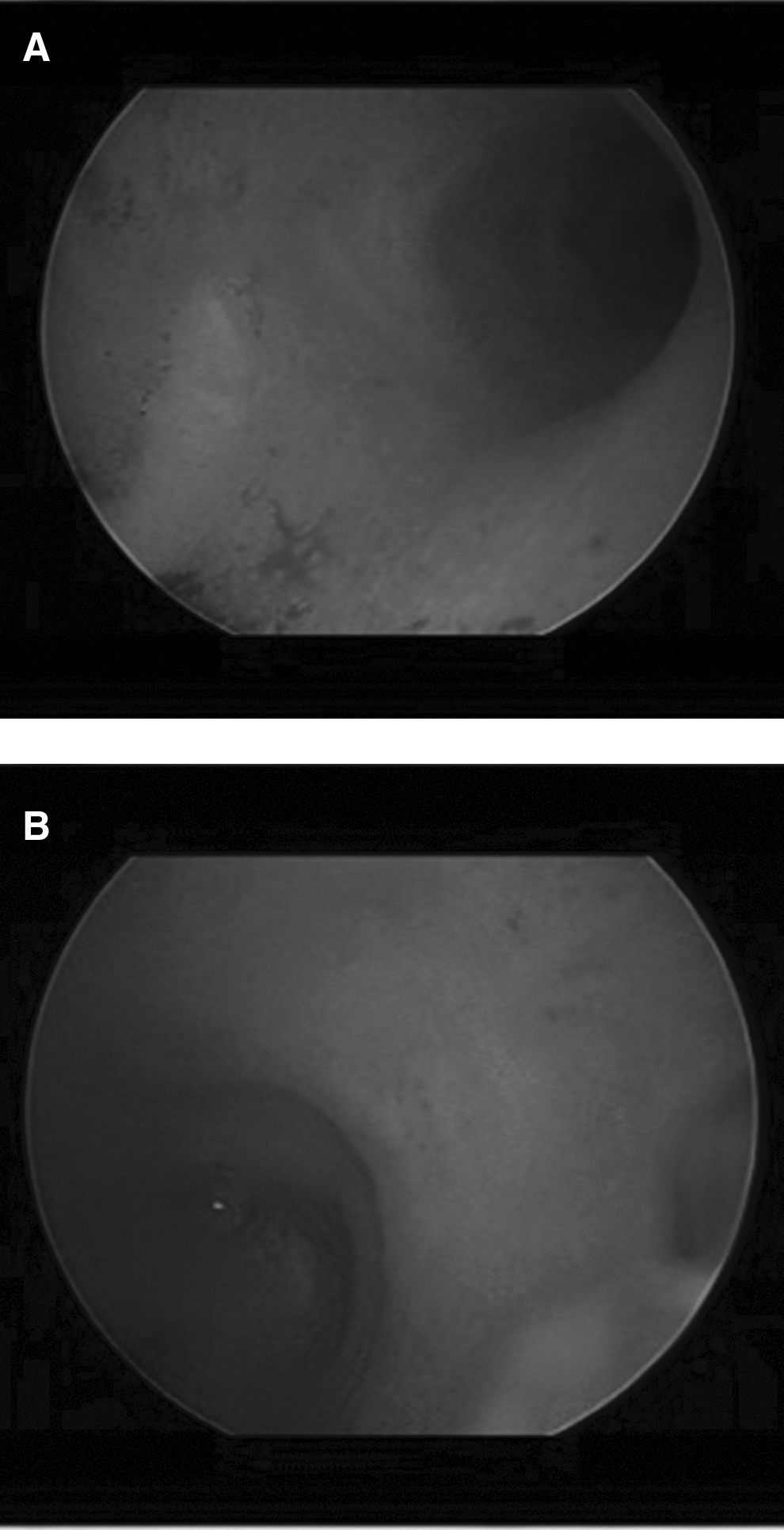

Hysteroscopic picture 18 months after laparoscopic myomectomy showing the fundal region after dividing an incomplete short uterine septum (1.5 cm in length at the mid-fundal region).
Results
The patient is currently trying to conceive.
Discussion
Removal of submucosal and intramural fibroids distorting the endometrial cavity has shown to improve fertility outcome. 6 Submucous fibroids are classified into three categories according to ESGE classification: type 0 if they pedunculate 100% into the uterine cavity; type I if they arise from the myometrium, but more than 50% of their mass is within the cavity; and type II if they arise from the myometrium, but less than 50% of their mass is within the cavity. 4 Lasmare et al. introduced a new classification of submucous fibroid. In this classification, four criteria were considered: the penetration of the nodule into the myometrium, the extension of the base of the nodule with respect to the wall of the uterus, the size of the nodule, and the topography of the nodule. 7 More recently, Lasmare et al. renamed the new classification STEPW. 8 In a multicentric study, they correlated ESGE and STEPW classifications with complete and incomplete hysteroscopic removal of a submucosal fibroid and concluded that STEPW permits a greater correlation. 8 With a score of 7 (STEPW classification), complete hysteroscopic removal was not possible.7,8
Hysteroscopic division of a uterine septum has been shown to improve the reproductive outcome in patients with RPL.1,9,10 Correction of a subseptate (septum ≥1.5 cm) or arcuate uterus (septum ≤1.5 cm) in women with prior pregnancy loss equally results in a significant decrease in rates of abortion.11,12
The real challenge in this case was the suspicion of a concurrent uterine pathology based on the hysteroscopic findings at the conclusion of the laparoscopic myomectomy. In fact, most practitioners will not perform a hysteroscopy, especially when the uterine cavity has not been entered. Practitioners should maintain a high index of suspicion whenever no cause for RPL is found. A review of the literature revealed no previous report on diagnosis or surgical management of a type II submucous fibroid coexisting with an incomplete uterine septum. This is therefore the first report of such an association. We believe that the ideal approach to this challenge is first to attend to the uterine leiomyoma via myomectomy and subsequently to perform hysteroscopic septal division after at least 3–4 months to allow for myometrial healing.
Conclusions
The coexistence of a type II submucous fibroid in the fundal region of the uterus and an incomplete uterine septum is indeed not only a diagnostic but also a surgical challenge. Removal of just the fibroid can still result in RPL. Surgical management of such coexisting uterine pathology cannot be performed in a single session.
Footnotes
Acknowledgments
The authors would like to thank Cheryl Anderson for preparation of this article. This abstract was presented at the Global Congress of Minimally Invasive Gynecology 40th Annual Meeting of the American Association of Gynecologic Laparoscopists (AAGL). J Min Invas Gynecol 2011;186:S154.
Disclosure Statement
No competing financial interests exist.