
Abstract
Abstract
Introduction
Case
A 22-year-old gravida 3 para 2 woman presented to the Department of Obstetrics and Gynecology as an emergency case with a history of amenorrhea for 39 weeks, watery vaginal discharge, and labor pains for 16 and 14 hours respectively. She was dehydrated and febrile (body temperature 100° F) with a pulse of 104 beats per minute and blood pressure of 100/60 mm Hg. A fetal heart rate of 96 beats per minute was audible. Catheterization of the urinary bladder revealed 20 mL of hemorrhagic urine. The abdomen was distended with a term-size gravid uterus with the fetus in cephalic presentation. The uterus appeared to be tonically contracted, and a Bandl's ring was apparent between the umbilicus and the symphysis pubis. The external genitalia were reddened and edematous. Vaginal examination revealed a dry vagina, a fully dilated cervix with the vertex at 0 station, and a large boggy caput and excess molding. Preliminary hematological and urine investigations were within normal limits. Ultrasonography revealed a term, healthy fetus and almost no amniotic fluid. After immediate resuscitation and informed consent, the woman was taken up for cesarean section.
At cesarean section, the urinary bladder was edematous and lifted up. The lower uterine segment was thinned out and distended. There was no evidence of blood in the peritoneal cavity. After mobilizing the urinary bladder, a lower-segment cesarean section was performed to deliver the baby. Difficulty was encountered in disimpacting the fetal head from the lower pelvis, and an assistant was asked to push the head from below. The 3.2 kg baby was delivered with an Apgar score of 2/10 and 7/10 at 1 and 5 minutes of birth respectively. However, immediately after delivery of the baby, the angles of the uterine incision could not be located, and a circumferential avulsion of the body of the uterus from the lower uterine segment was detected (Fig. 1). Both the broad ligaments were also torn up to a level just below the attachment of the fallopian tubes and ovarian ligaments to the uterus. Application of hemostatic clamps on the avulsed margins of both sides helped reduce the profuse hemorrhage that followed. The uterine vessels on both sides were ligated below the site of avulsion. Consent for hysterectomy was obtained, and a total hysterectomy was carried out. Continuous urinary drainage was done for 10 days. The woman and the baby fared well postoperatively and were discharged after 7 days.
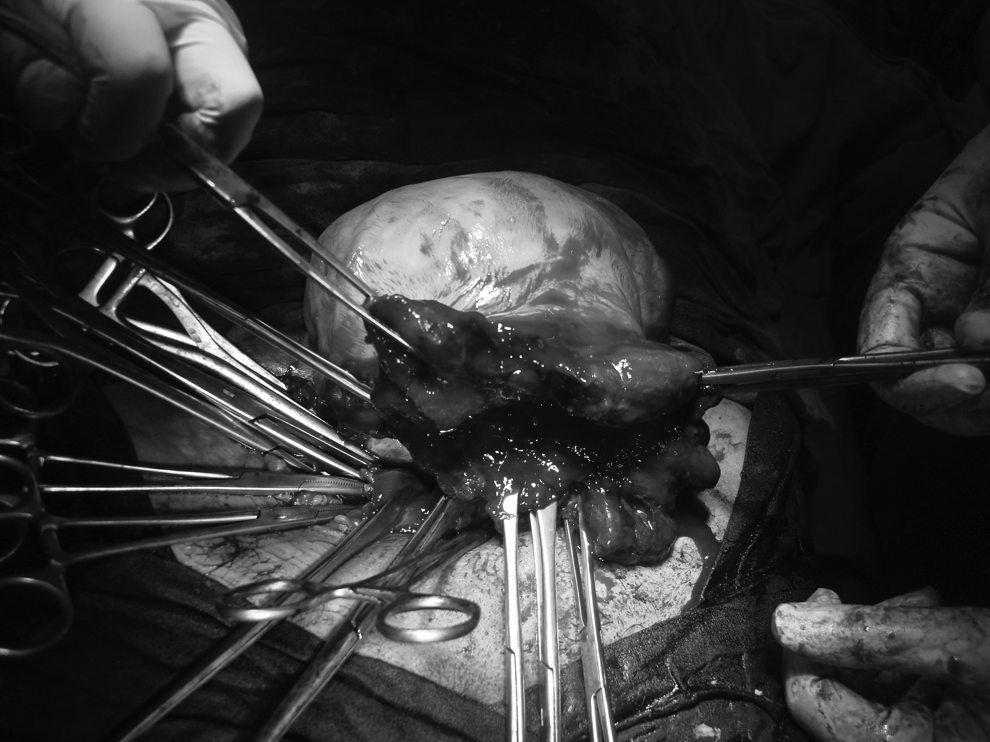
Intraoperative photograph during cesarean section showing complete avulsion of the body of uterus from the lower uterine segment.
Discussion
Cesarean section with a deeply engaged fetal head accounts for about 25% of all emergency cesarean sections. 1 Obstructed labor still continues to be a major cause for this in developing countries, while in developed ones failed instrumental delivery accounts for most of them. In addition, a cesarean section can also be the result of a deep transverse arrest, arrest in the occipitoposterior position, and unanticipated cephalopelvic disproportion in late labor. A reluctance to resort to instrumental delivery, particularly rotational forceps, in the late second stage of labor may further add to the numbers. 1
In the present case of obstructed labor, the uterus was tonically contracted over the fetus. An overstretched lower uterine segment in this multiparous woman was already predisposed to rupture as a result of obstructed labor. Pushing up the fetal head by an assistant, coupled with the difficulty the surgeon encountered to reach below the presenting part, which was compounded by the absence of amniotic fluid, probably resulted in the lower segment incision extending itself laterally and then posteriorly to cause the complete avulsion. The extension of the incision involved both broad ligaments and uterine vessels, resulting in significant hemorrhage. However, since the complication was recognized immediately, the blood loss was significantly less than what would be evident in a laparotomy done for a ruptured uterus. The vital parameters of the woman remained stable, and a total hysterectomy was carried out.
Pushing up the fetal head by an assistant cannot only cause direct trauma to the head but can also delay the uterine incision to delivery time. 4 It may also cause extension of the uterine incision, particularly if performed during a contraction. In a uterus with an advanced Bandl's ring, as in the present case, the thinned out lower uterine segment is already on the verge of rupture, and this can be precipitated by pushing up the fetal head from below.
A head-down tilt, an abdominopelvic approach, breech extraction of the baby, and use of the fetal disimpacting system have all been proposed in an effort to lessen the incidence of maternal and fetal complications in cases of wedged fetal head during cesarean section. 5 However, none is effective in all women, and cases need to be assessed individually. Nevertheless, a Trendelenburg position and preferential use of the pull-out method by an experienced surgeon can help decrease the complications of this difficult cesarean delivery. Also, all cesarean sections in the advanced second stage of labor should be either carried out by experienced obstetricians, or at least a consultant should be present in the operating room so that they can take over the procedure immediately in the event of difficulty.
Footnotes
Disclosure Statement
No competing financial interests exist.