
Abstract
Abstract
Introduction
We report a case of abdominal/pelvic splenosis presenting with chronic abdominal pain, successfully treated by laparoscopic excision.
Case
A 45-year-old Caucasian female (gravida 1, para 1) presented at gynecological clinic with a history of 2 years of chronic pelvic pain and more recently postcoital bleeding. She had a history of splenectomy during her childhood due to traumatic rupture during a car accident. Her medical history was unremarkable, with a surgical history comprising one cesarean section.
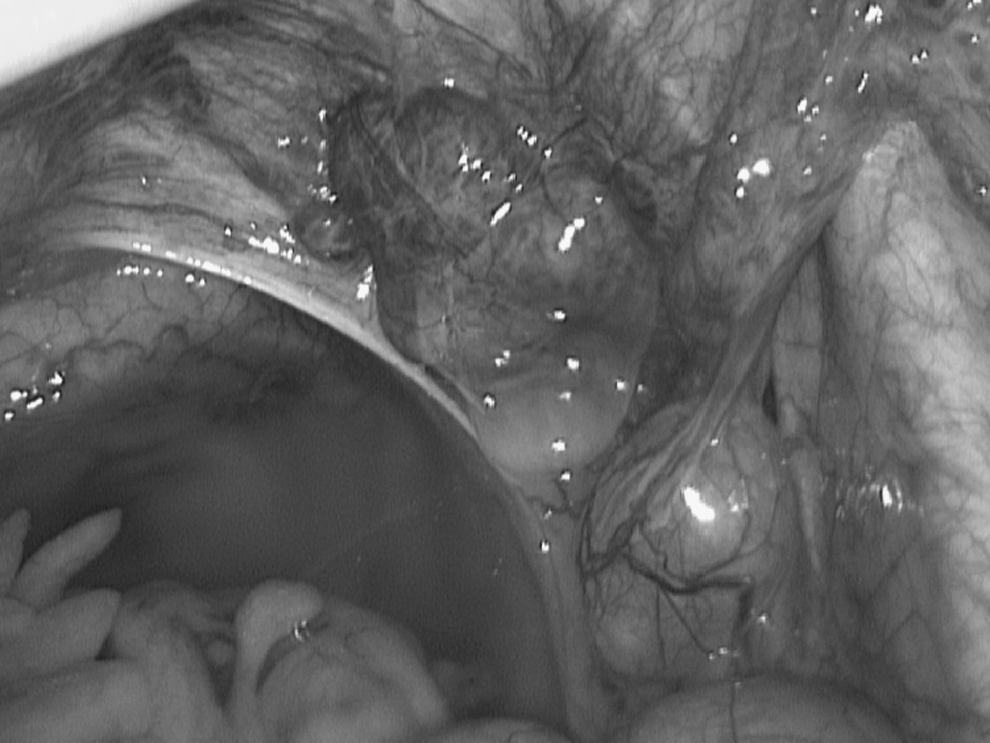
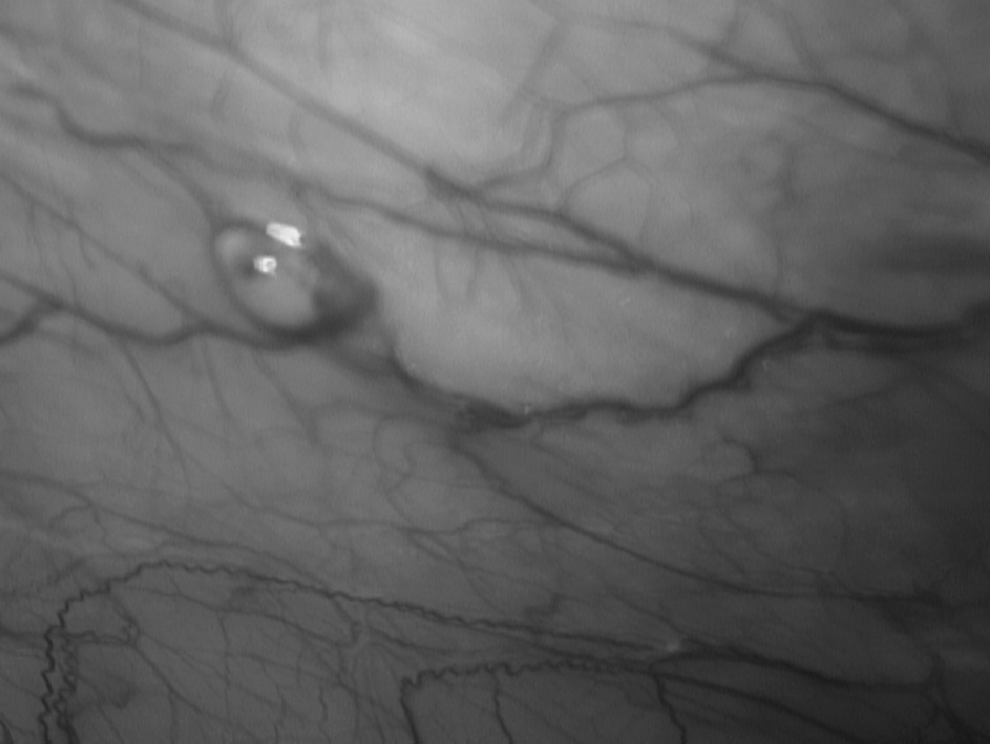
During the pelvic examination, the uterus was found to be antiverted, normal in size, and not tender, but the right adnexa was found to be tender. A transvaginal ultrasound (TVS) showed two unilocular pelvic masses with regular well-defined borders and homogeneous low-level echoes measuring 21×16×17 mm and one similar lesion measuring 31×13×32 mm, both adjacent to the right ovary. No pelvic fluid was noted. The uterine cavity and the endometrium were unremarkable. The result of the ultrasonography examination was a suspected endometrioma. An endometrial specimen taken during her examination in the gynecological outpatient clinic revealed a perimenopausal endometrium. Serum tumor marker cancer antigen 125 (CA-125) was 7 IU/mL and carcinoembryonic antigen (CEA) was 1 IU/mL. To investigate the pelvic masses further, an abdominal and pelvic magnetic resonance imaging (MRI) scan was requested. This revealed a possible fimbrial cyst measuring 2.2×2.7 cm near the right ovary and a tubular mass measuring 3.8×1.8 cm adjacent to the fimbrial cyst. The conclusion from the MRI was of possible tubal cancer. Before the operation, the patient was advised of the various surgical options, such as either cystectomy or oophorectomy or salpingectomy or even hysterectomy, according to the findings during surgery. On laparoscopy, a normal-size uterus adherent to the anterior abdominal wall was seen. On the right ovarian fossa, a bluish-red 4×5 cm mass was found (Fig. 1). The cul-de-sac was crowded with small and same-colored masses ranging in diameter from 0.5 to 2 cm. Two additional masses were noted on the serosal surface of the abdominal cavity just under the diaphragm (Fig. 2). There was no evidence of endometriosis or ascites, and both ovaries were normal. The excision of the macroscopic lesions was performed using monopolar scissors, and the specimen was placed intact inside an endoscopic bag before being extracted. Final histopathological examination revealed splenic tissue, and diagnosis of pelvic splenosis was determined. The patient made an uneventful recovery, and she was discharged the same day. At 6 months following surgery, she was free from abdominal pain.
Pelvic splenosis.
Pelvic splenosis.
Discussion
Splenosis following traumatic splenectomy after a traffic accident is well documented in the literature, but the minority of these are gynecological cases.9–16 Autotransplantation of splenic nodules following spleen trauma has been described in all intraperitoneal and some extraperitoneal sites as well. 17 Splenectomy for nontraumatic reasons may also lead to splenosis if splenic tissue is spilled on the peritoneal surface at the time of surgery or if morcellation extraction of the spleen is used during laparoscopic splenectomy, as reported by some authors. 18
Presentations of the implants can be quite varied, ranging from asymptomatic to acute abdominal pain with intraabdominal hemorrhage 19 to bowel obstruction. 20 Pleurisy and hemoptysis have been described, as they may be the presenting symptoms when thoracic splenosis occurs. 21 Our patient complained of chronic abdominal pain, which was affecting her daily life. The average reported interval between the spleen trauma and the diagnosis of splenosis is 19 years, but in our patient there was 25-year interval between splenectomy and final diagnosis. In our patient, the presumed diagnosis could have been made using the patient's history of prior splenectomy or at least of severe abdominal trauma. Diagnosis can also be made by the absence of siderocytosis and Howell–Jolly bodies in the blood smear of a patient with history of splenectomy. 19 Moreover, the majority of the patients with splenosis are asymptomatic, and therefore the diagnosis is incidental with ultrasonography (USS), computed tomography (CT), or MRI examinations. Splenic implants can also be diagnosed with scintigraphy study using heat-damaged Tc-99m-labelled autologous red blood cells, as described by some authors.22,23 At laparoscopy, these implants are usually bluish in color and have no hilus, supplied by local arteries that penetrate their fibrotic capsule. Splenosis may mimic endometriosis or benign or malignant pelvic cancer, as happened initially in our patient and as described by other authors. 6 According to the same authors, 6 a lack of adhesions and spread within the peritoneum would suggest splenosis rather than endometriosis. Furthermore, splenosis differs in color and consistency from malignant tumors and in consistency from fibroids. Splenosis should also be distinguished from accessory spleen, which is a common finding in autopsies, and which is usually single and is supplied by a branch of the splenic artery. 19 The conclusive diagnosis has to be by histological report, as we did in our case.
Management of splenosis depends on patients' symptoms. In general, it is accepted that asymptomatic implants should not be removed because these splenic nodules may be immunologically functional and thus useful for the patient. It has been reported that the overall incidence of sepsis and mortality is significantly higher in cases of incidental splenectomy than in cases of posttraumatic splenectomy. Furthermore, excision of splenic nodules may cause injury of the vital organs to which they are attached. Therefore some authors argue that symptomatology is the key issue. 16 In our case, the patient was symptomatic, and therefore the decision was to remove the spots of suspected splenosis, especially because complications by torsion and hemorrhage of infection have been reported. 13 During surgery, the implants of suspected splenosis were removed using monopolar scissors, which resulted in a successful removal without violating the splenic capsules and minimizing bleeding and time of dissection. We are aware that even resection with argon bean coagulator has been described. 24 At the time of the surgery, the rest of the pelvic and abdominal organs were unremarkable, and therefore we did not feel it necessary to remove the ovaries or the tubes. The laparoscopic approach allowed the patient to be discharged the same day.
Conclusion
In conclusion, splenosis must be considered in the differential diagnosis of previously splenectomized patients who present with unexplained masses and/or chronic or acute pelvic pain, especially in the context of a history of trauma and splenic rupture. Minimally invasive surgery via laparoscopy is ideal for the diagnosis and treatment of such patients.
Footnotes
Disclosure Statement
No competing financial interests exist.