
Abstract
Abstract
Introduction
Case
In 2002, a 55-year-old, gravida 6 para 4 woman with a family medical history of colorectal adenocarcinoma and a past medical history of diabetes mellitus and hypertension presented with postmenopausal bleeding. Pelvic examination under anesthesia was normal; specifically, no parametrial involvement and no tumor were seen in the cervix. She underwent endocervical curettage and endometrial biopsy, which confirmed a grade 1 adenocarcinoma in the endometrial specimen. After pelvic examination and histological biopsy, the patient was diagnosed with endometrial adenocarcinoma FIGO stage I. Initially, the patient refused to undergo surgery, so she was treated with a low-dose rate brachytherapy (10 Gy, Ir-192). Thereafter, she agreed to surgery, and a total abdominal hysterectomy, bilateral salpingo-oophorectomy, and lymph node dissection were carried out, including 11 pelvic and 8 paraaortic lymph nodes. Histologic examination revealed an infiltration of two thirds of the myometrium but did not reveal any malignant involvement of the lymph nodes, although some of them showed a modified architecture. The tumor was classified as FIGO stage IB grade 1, and due to the initial brachytherapy and the modified architecture of some lymph nodes, the patient received fractionated external beam radiotherapy, with a total dosage of 50 Gy (2 Gy day−1, 5 day week−1, for 5 weeks). The patient showed no evidence of recurrent disease during the following years until she presented in December 2011 with postmenopausal bleeding. Histologic examination of the vaginal vault revealed a moderately differentiated squamous cell carcinoma (Fig. 1). Chest, abdominal, and pelvic computed tomography (CT) scans did not show any distant metastases, but the lesion was not amenable to carcinologic surgery; in fact, according to our surgical department, complete removal of the tumor with negative margins in this previous radiation field was not possible, and once again the patient was reluctant to even consider the possibility of having more surgery. Therefore, she received a 3-weekly chemotherapy regimen based on 5-fluorouracil (1,000 mg/m2 d1–d5) and cisplatin (100 mg/m2 d1). After four cycles of this regimen, the tumor had increased in size on the control CT scan. To date, the patient is still alive with a progressive disease, and she still receives symptomatic treatment.
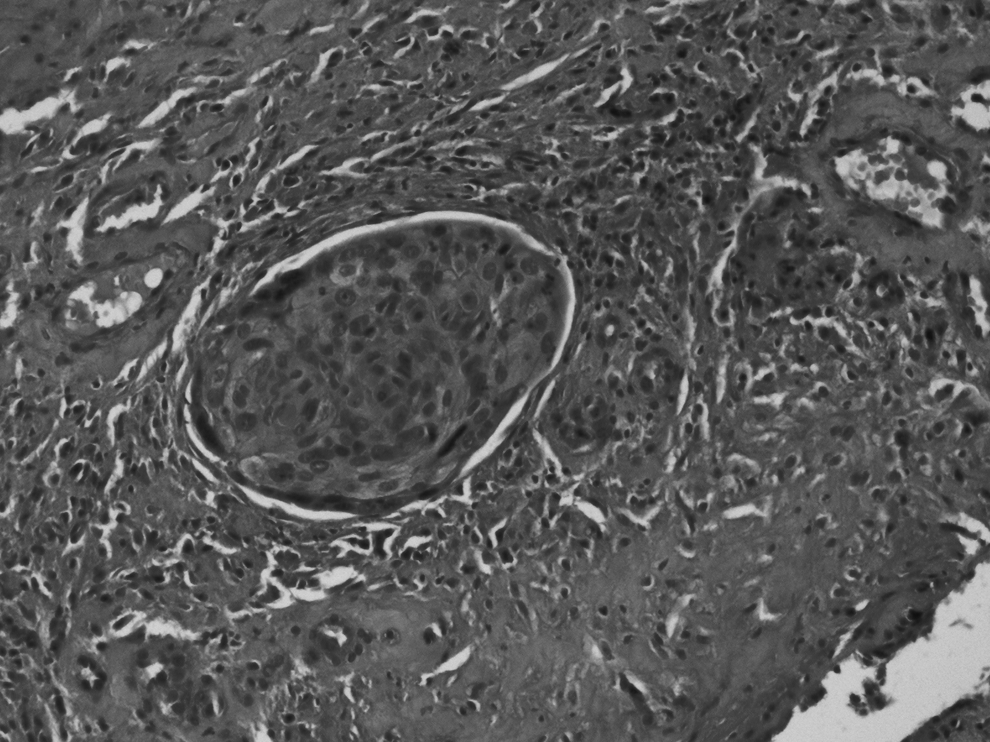
Microscopic image of vaginal squamous cell carcinoma.
Discussion
Since the use of radiotherapy for the treatment of malignant conditions, there have been numerous studies that have attempted to evaluate the carcinogenic effect of radiation on various organs, especially those located in close proximity to the irradiated field. Lorigan et al. 4 suggested that for radiation to induce malignant change, the injury to individual cells must be sufficient to cause genetic mutation but insufficient to cause cell death; such situations can arise within and at the margin of the radiation field. In fact, radiation therapy has been reported to increase the risk of lung cancer after breast irradiation, 5 breast cancer after irradiation for Hodgkin disease, 6 thyroid cancer after neck irradiation, 7 ovarian and endometrial cancer after pelvic irradiation, 8 and salivary carcinomas after head and neck irradiation. 9 However, and to our best knowledge, vaginal cancer following irradiation for endometrial cancer has not been reported previously, but vaginal cancer after radiotherapy for cervical cancer has been widely described.10–14 More recently, based on 12,496 second cancers in a population-based study of more than 100,000 cervical cancer patients, Chaturvedi et al. 2 reported that following radiotherapy for cervical cancer treatment, risk for all second cancers at sites in close proximity to the cervix (rectum/anus, colon, urinary bladder, ovary, and female genital sites other than the cervix) continued to increase over time and remained elevated for more than 40 years.
However, the concept of postradiation carcinoma is not widely appreciated and has not been adequately defined by clinicopathological study. 3 A simple causal relationship between radiation and subsequent carcinoma is more complex: vaginal and vulvar carcinomas are related to human papillomavirus (HPV), and it is possible that HPV infection or reinfection rather than radiation is the predisposing factor in those patients whose postradiation tumors are also HPV related. 3 In fact, when carcinoma of the vagina develops in a patient treated previously for other pelvic tumors with radiotherapy, there is always the question of whether it represents a new radiation-induced tumor or a late recurrence of the disease. Most authors use the limit of an interval of 5 years or more and cytological smears to differentiate primary from secondary vaginal carcinoma.14,15 Also, the diagnosis of radiation-associated vaginal cancer is still difficult due to the lack of specific symptoms in most cases. In fact, x-ray therapy usually induces cervical stenosis and obliteration of the upper vagina, leading to negative cytology and the prevention of vaginal bleeding.16–18 Colposcopic examination of the vagina may also at times be nonproductive, as the lesion may not be delineated owing to radiation atrophy. 13 Particular attention should be directed to the angles of the apex of the vagina, as they are often the hidden sites of carcinoma, and such areas are difficult to examine and biopsy. Also, there tends to be a long latent period between the appearance of the secondary malignant tumors and the initial irradiation—sometimes more than 10 years with a median of 16 years.16,17,19,20 Therefore, some patients could neglect to relate the secondary malignant tumor to their prior irradiation. This delay in diagnosis could explain the high proportion of advanced cancers 20 and the worse prognosis of such tumors.
In a retrospective study conducted by Senkus et al. 21 concerning 35 radiation-induced squamous cell carcinoma of the vagina or the vulva, 24 tumors were located within the high dose volume and 11 within the scattered irradiation area. The time span between pelvic irradiation and vaginal/vulvar cancers ranged from 79 to 402 months (median 219 months). This interval between pelvic irradiation and the secondary tumors is considerably longer than the median time to local recurrence of cervical cancer. Senkus et al. did not objectify any correlation between second tumor stage and intensity of the previous pelvic irradiation. In another retrospective study conducted by Choo et al., 13 which included 29 second neoplasms in the vagina following radiotherapy for cervical cancers, the mean interval to the development of vaginal invasive carcinoma was 22.7 years. Our patient was 55 years old when she was treated for her endometrial cancer with radiotherapy, and she developed a radiation-induced vaginal cancer 10 years later. This interval is as reported in the literature. In fact, young patients who are treated with radiotherapy live long enough to develop a second neoplasm in the irradiated field, and thus life-long surveillance in this group of patients is mandatory.
On the other hand, some authors have suggested that postirradiation carcinomas are usually poorly differentiated and among the most aggressive subtypes.3,22,23 Therefore, and in contrast to sporadic tumors, secondary cancers following radiotherapy may require more aggressive surgical staging and adjuvant treatment. Also, this treatment should be individualized, taking into consideration the patient's age, type of malignancy, extent of disease, previous therapy, and the need to preserve sexual function. Modalities of treatment for vaginal radiation-induced carcinoma were quite different based on radical surgery or exenteration, radiotherapy, or palliative chemotherapy.13,15,21 Senkus et al. 21 reported that the intent of treatment for a secondary tumor and the stage of the secondary tumor did not represent significant prognostic factors. 21 In fact, it is difficult to assess precisely the disease extent of the secondary tumor in irradiated tissues, and this could explain in some extent the lack of influence of tumor stage on survival.
The prognosis of radiation-induced neoplasms is usually worse than that for spontaneous disease. Senkus et al. reported a median survival of 52 months in their study, which includes 35 vaginal and vulvar carcinoma following pelvic radiotherapy among 46 patients. 21 The poor prognosis may be explained by the significant delay in diagnosis, the advanced stage of illness, the aggressive histology subtypes and high grade of such radiation-induced tumors,18,21,22 and the modalities of treatment; in fact there is a high number of patients that receive only palliative treatment due to difficulties in performing another aggressive therapy following previous radical surgery and/or radiotherapy. Due to the fear of complication, the intent of treatment for a secondary pelvic tumor is, in most cases, palliative. 24 Another problem was inadequate compliance of patients who, like our patient, had often suffered from late sequelae from first treatment and were reluctant to be exposed to another radical approach.
Conclusion
Clinicians and pathologists should be aware of the potentially increased risk not only of soft tissue sarcomas but also of carcinomas in patients with a history of pelvic radiation therapy. To detect possible occult malignancy as early as possible and given the latent period of one or more decades, a long-term follow-up and an aggressive investigation, even including tissue biopsy, are mandatory whenever patients with a past medical history of previous irradiation experience any pelvic symptoms. Patients should be observed closely, and it is important to continue careful annual surveillance, even if the patient has been free of disease for many years, as secondary malignant tumors tend to have a long latent period.
More aggressive treatment may be considered for these patients to improve prognosis: radical treatment, whenever it is possible, would be applied more frequently than palliative treatment.
Footnotes
Disclosure Statement
No competing financial interests exist.