
Abstract
Abstract
Introduction
Cases
Case 1
A 37-year-old woman with no significant past medical history presented with a painless lump in the upper-outer quadrant of the right breast, which had been noticeable for 7 months and had progressively increased in size. Physical examination revealed a 40-mm, well-circumscribed, painless, mobile, and firm mass, with no evidence of axillary lymphodenopathy. Mammography showed a 35-mm, circumscribed, and hypodense mass without microcalcification. This lesion was classified as ACR 3 (American College of Radiology). On ultrasonography, the lesion was well circumscribed, parallel in orientation, hypoechoic, and solid with moderate acoustic enhancement. No enlarged axillary lymph nodes were noted. Although the mammography and ultrasonography findings indicated that the mass was benign, the patient chose to have the tumor excised rather than conservative follow-up. Macroscopically, the tumor measured 36 mm and was encapsulated, firm, homogenous, and whitish on section. Histological examination revealed spindle cells, often arranged in a palisading fashion or in an organoid arrangement. No atypical mitotic figures were present. The tumor was diffusely immunoreactive for S-100 protein and negative for desmin, cytokeratin, and CD34. Based on these findings, a histopathological diagnosis of schwannoma of the breast was made. At 5 years of regular follow-up, the patient did not show any evidence of recurrent disease.
Case 2
A 31-year-old female with no significant past medical history complained of a mass that had been growing slowly in her left breast for more than 3 years. Clinical examination revealed a 50-mm, well-circumscribed, and firm mass at the union of external quadrants. There were no signs of nipple discharge, skin changes, or regional lymphadenopathy. Mammography showed a well-defined and dense nodule without microcalcification, visible only on the angled side view. Supplementary ultrasonography showed a 45-mm, hypoechoic, heterogeneous, and well-defined mass, which corresponded to the mammographic abnormality and the clinically palpable lump. These findings suggested a benign lesion. Options of ultrasound-guided core needle biopsy and surgical excision were discussed, and the patient subsequently had a surgical excision, and a 42-mm, well-defined mass was removed. The cut surface was homogenous and the specimen was yellowish white. Hematoxylin-eosin staining showed fascicles of fusiform cells with elongate nuclei and indistinct cytoplasmic borders, which were often arranged in a palisading pattern. The tumor was diffusely immunoreactive for S-100 protein and negative for desmine, CD34, and cytokeratine. There were no atypical cells, and no mitosis was observed. Based on these findings, a histopathological diagnosis of schwannoma of the breast was made. At 3 years of regular follow-up, the patient did not show any evidence of recurrent disease.
Case 3
A 29-year-old asymptomatic female with a past medical history of bilateral breast adenofibroma treated with surgery 3 years ago presented with a palpable lump in her left breast. She first noted it 2 weeks prior on self-examination. She had no family history of breast carcinoma. Clinical examination revealed a 30-mm, well-defined, firm, and mobile lump in the left lower outer quadrant. No mass was detected on mammography but sonography revealed a 25-mm, well-defined, hypoechoic, and deep located mass with homogenous internal echo within the breast. Subsequently, the patient had a surgical excision. A well-encapsulated firm mass was removed, and it measured 25 mm and was yellowish white on cross-section. Histological examination revealed a benign mesenchymatous proliferation: spindle-shaped cells with poorly defined eosinophilic cytoplasm and pointed basophilic nuclei, set in a variably collagenous stroma (Antoni A tissue). Areas of cells with parallel arrays of nuclear palisading known as Verocay bodies were noted on high power. On immunohistochemical staining, the tumor cells were positive for vimentine and S-100 protein, consistent with a diagnosis of schwannoma. At 2 years follow-up, the patient was doing well with no recurrence.
Case 4
A 32-year-old woman presented with a 1-month history of a left breast mass. A physical examination revealed a 15-mm, well-limited, elastic-soft, smooth, and mobile mass in the upper left breast. There was no evidence of axillary lymphadenopathy. On screening mammogram, the lesion appeared as a circumscribed, round-oval, and equally dense nodule without microcalcifications. Ultrasonography revealed a 20-mm, oval-shaped, hypoechoic, and heterogeneous mass with moderate acoustic enhancement (Fig. 1). The tumor was hypocascular on color Doppler with a 10-mm inflammatory enlarged axillary lymph node. Although, these findings suggest that the mass was benign, a surgical excision was performed under local anesthesia. Macroscopically, the mass was well defined and oval-shaped, measuring 20 mm, and was entirely covered by a thin, whitish capsule. A microscopic examination revealed a structure of interlacing bundles of numerous elongated spindle-shaped cells, arranged in a palisading pattern with occasional Verocay bodies (Fig. 2). No atypical mitotic figures were present. Immunohistochemically, the tumor cells exhibited intense staining for S-100 protein (Fig. 3). These findings were compatible with schwannoma. At 2 years of regular follow-up, the patient was doing well with no evidence of recurrent disease.
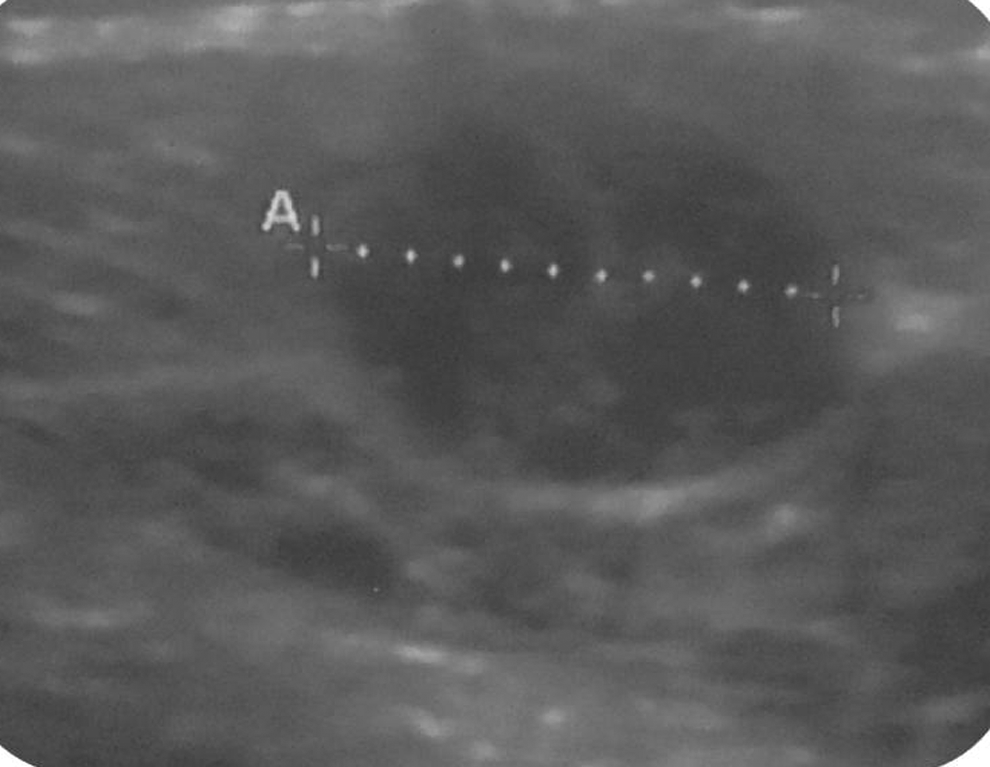
Ultrasonography showed a well-circumscribed heterogeneous and hypoechoic mass.
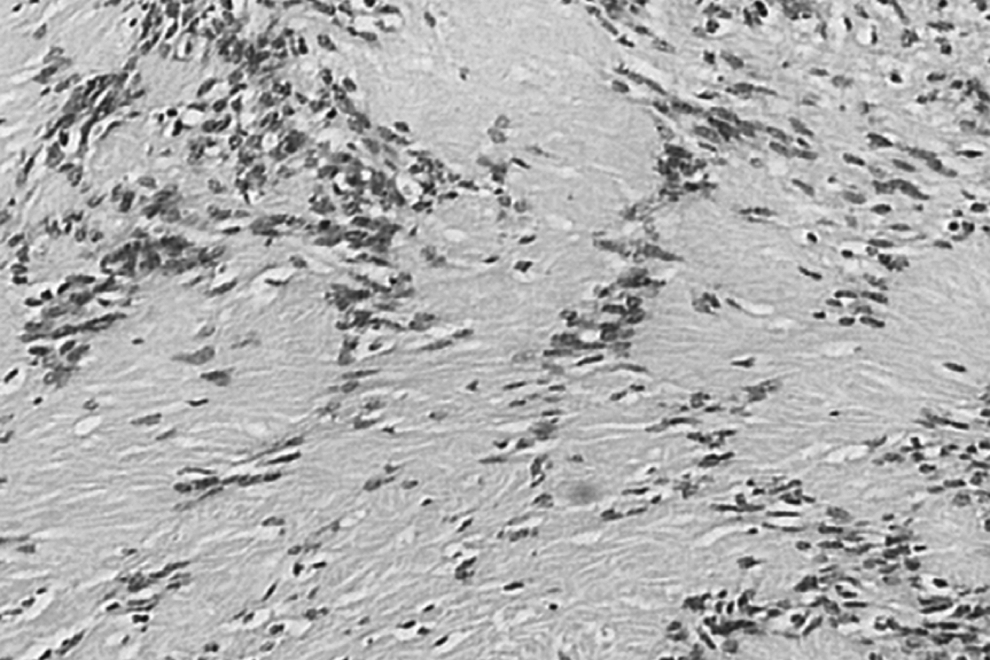
Areas of spindle-shaped cells with parallel arrays of nuclear palisading known as Verocay bodies.

S-100 protein staining was positive in the tumor cell cytoplasm.
All patients in this case series were still alive at the time of preparing this report and did not show any evidence of recurrent disease at their regular follow-up.
Discussion
Schwannoma is a benign and slow-growing tumor that usually arises on peripheral nerves or spinal roots.1,2 Neurilemoma, neurinoma, and schwannoma are considered to be synonymous. Any part of the body can be affected, but the most common locations include the head, neck, and extensor surfaces of the extremities. 3 However, the localization in the breast is very unusual and accounts for only 2.6% of schwannomas according to Das Gupta et al. 4 To the best of our knowledge, only 29 previous cases have been reported in the literature. The clinical features of the all cases, including those of our case, are reported in Table 1.1–3,5–23 Twenty-seven patients were female and six were male, and the patients ranged in age from 18 to 83 years, with a mean age of 45.9 years. The tumors were most often located in the upper outer quadrant following by the upper inner quadrant. The tumor size ranged from 0.7 to 11 cm with a mean size of 3.5 cm.
Q=quadrant involved; F=female; M=male; R=right; L=left; U=upper; Lo=lower; UO=upper outer; LI=lower inner; UI=upper inner; O=outer; AT=axillary tail; C=central; NS=not specified.
Mammographic and ultrasound findings in schwannoma of the breast have not been widely described due to the rarity of this entity. Mammographically, schwannomas are most commonly described as a nonspecific, well-defined, round or oval, and equally dense nodule.1–3,12,16,18,23 Also, a normal mammogram without any detectable mass,17,20 and an ill-defined area of dense soft tissue 15 have been reported. In our cases, the mammographic findings were similar to those reported previously. In fact, in one patient, the mammography was normal, and in the other three patients, the lesion appeared as a circumscribed, round-oval, and dense nodule without microcalcifications. On ultrasonography, more variation in appearance has been reported. However, it is most commonly reported as a solid hypoechoic, well-defined mass of benign appearance with variable posterior acoustic enhancement.1,3,12,16–18,20,23 Also, a cystic degeneration has been reported. 2 For these reasons and based solely on imagery, it can be very difficult to distinguish schwannoma in the breast from other benign or malignant tumors.
Microscopically, classic schwannoma is an encapsulated neoplasm and consists of two alternating components in variable proportions known as Antoni A tissue and B tissue. Antoni A tissue is an organized cellular component and consists of monomorphic spindle-shaped Schwann cells, with poorly defined eosinophilic cytoplasm and pointed basophilic nuclei, set in a variable collagenous stroma. 2 These cells commonly form a palisading arrangement known as Verocay bodies. Antoni B is a relatively less cellular component and contains more loosely arranged cells.24,25
Given the histological characteristics of breast schwannoma, the differential diagnosis from other lesions showing spindle cells may be difficult and includes phylloides tumor, fibroadenoma with minor epithelial components, fibromatosis, neurofibroma, myoepithelioma, myofibroblastoma, and metaplastic carcinoma.1,2 However, immunohistochemically, schwannoma cells exhibit intense and uniform staining for S-100 protein, 21 which helps to establish an accurate diagnosis.
A cytological diagnosis of schwannoma of the breast may be possible by fine-needle aspiration cytology.1,2 However, schwannoma of the breast is such an infrequently encountered tumor that fine-needle aspiration cytology may not result in a correct diagnosis in some cases, 2 and in such cases a surgical excision is recommended. Primary malignant schwannomas of the breast have also been reported,26–29 and these tumors showed a benign appearance on imagery, and fine-needle aspiration cytology revealed atypical mesenchymal cells.27,28 Due to the rarity of breast schwannoma, the large differential diagnosis, and the possibility of underestimating a malignant entity, all our patients underwent a surgical excision rather than a fine-needle aspiration.
Adequate treatment of solitary benign schwannoma consists of simple enucleation of the encapsulated tumor. To date, recurrence after surgical excision has not been reported.
Conclusion
We have presented four cases of schwannoma of the breast and reviewed the literature. These tumors are usually well circumscribed, noninvasive, and usually show a benign appearance on imagery. A complete surgical excision of this lesion helps in making the definitive diagnosis, and represents the best choice of treatment.
Footnotes
Disclosure Statement
No competing financial interests exist.