
Abstract
Abstract
Introduction
Case
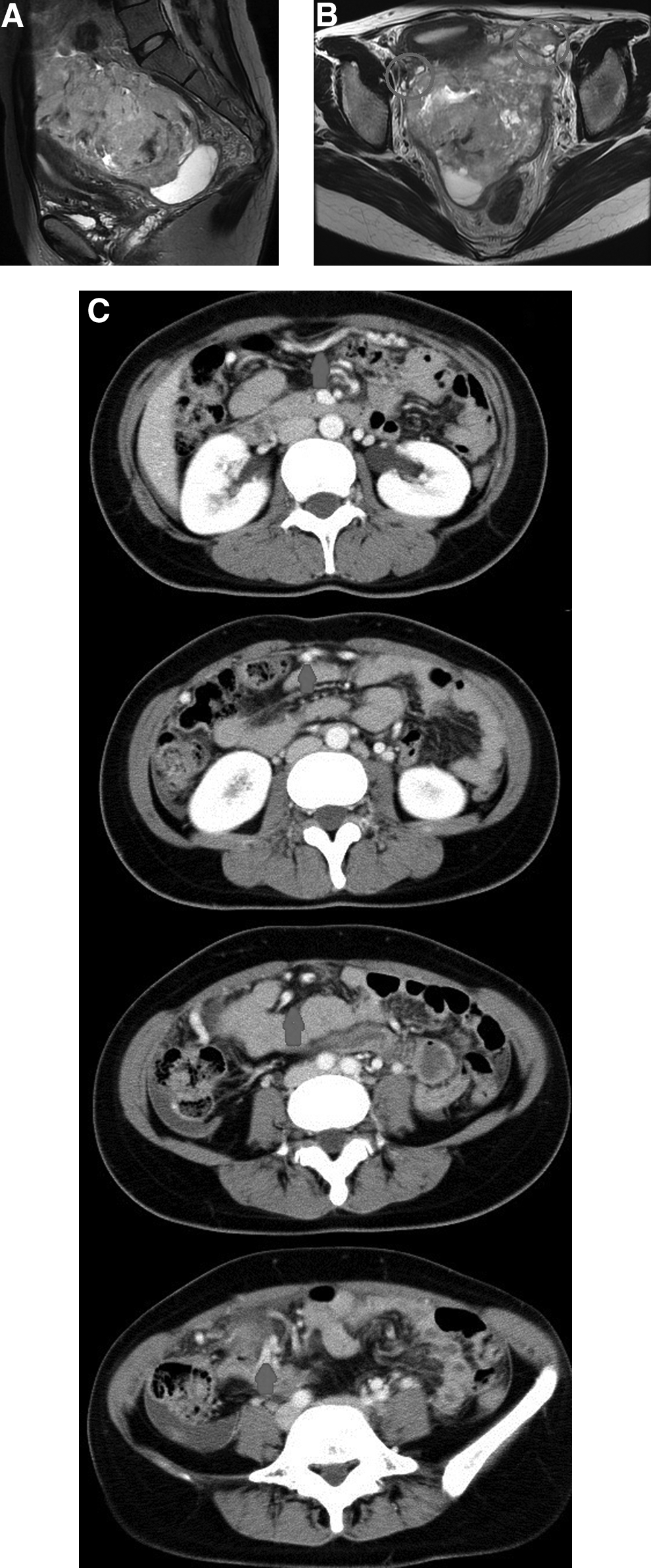
A 34-year-old, gravida 2, para 2, Japanese woman visited a previous hospital with the symptom of abdominal distension. Her medical and gynecological history was unremarkable. She menstruated regularly at 28-day intervals with normal flow volumes. At the hospital, she was examined with magnetic resonance imaging (MRI) and serum tumor markers. Serum alpha-fetoprotein (AFP) was elevated to 103,200 ng/mL (normal range: <6 ng/mL). Pelvic and abdominal MRI showed a solid, heterogeneous mass occupying the whole abdominal cavity with ascites (Fig. 1A). Both ovaries appeared normal in shape and size, and the tumor was adhered dorsal to the uterus. A YST arising from the uterus or an extragonadal YST was suspected (Fig. 1B). Abdominal and pelvic contrast-enhanced computed tomography (CT) imaging showed the tumor to be well vascularized. The main arterial supply to the tumor was from a branch artery of the gastroepiploic artery, which was dilated. This suggested that the main tumor-feeding artery came from the omentum (Fig. 1C).
After these examinations were done, she visited our hospital. On pelvic examination, an immobile, solid mass was palpated from the pelvis to the upper abdomen above the umbilicus. Pelvic ultrasonography showed a 16.6×92.3 mm heterogeneous hyperechoic mass. Serum CA-125 level was elevated to 308.2 U/mL (normal range: <35 U/mL), but serum CA19-9 and carcinoembryonic antigen levels were within the normal range. At the first exploratory laparotomy, a large, friable, and hemorrhagic tumor occupying the pelvis was found with 1.5 L of bloody ascites. The tumor was rigidly adhered to the intestine, dorsal uterus, and omentum. The tumor was so large that we suspected it infiltrated the intestine, and there was a risk of extensive bleeding in trying to resect the tumor. Thus we could resect only a small volume of tumor and could not identify its primary site.
Postoperative histological examination of the specimen exhibited the papillotubular, reticular, and solid proliferation of atypical cells with pale abundant cytoplasm. Many Schiller–Duval bodies were observed (Fig. 2A). Immunohistochemistry showed that the tumor cells were positive for AFP (Fig. 2B). Histological diagnosis of the resected specimens was YST. Other germ cell tumors were not included in the specimens. The tumor was designated as pT3cNXM0, FIGO stage IIIc. Two weeks after the primary surgery, the woman underwent combined intravenous chemotherapy under the bleomycin, etoposide, and cisplatin (BEP) regimen with bleomycin (15 mg/body on days 2, 9, and 16), etoposide (100 mg/m2 for 5 consecutive days), and cisplatin (20 mg/m2 for 5 consecutive days) every 3 weeks for four cycles. After four cycles, serum AFP dropped to 48 ng/mL. The woman was reexamined using pelvic and abdominal MRI, which showed shrinkage of the tumor. However, the largest tumor, which measured 8 cm, still remained in the pelvis. We then performed secondary cytoreductive surgery. At laparotomy, an 8-cm multilobulated solid mass adhered to the omentum was found. The uterus and both adnexae appeared grossly normal. Resection of the mass, excision of the small nodule located in the Pouch of Douglas and the serosa of the rectum, infracolicomentectomy, total abdominal hysterectomy, and a bilateral salpingo-oophorectomy were performed.

Overall, the cut surface of the tumor showed a solid mass with focal hemorrhage and cystic change (Fig. 3A). Microscopically, the tumor largely consisted of the degenerated tumor cells and necrosis surrounded by foamy macrophages with no residue of viable tumor cells, indicating a histologically complete response of the tumor to chemotherapy (Fig. 3B). Viable tumor cells were not observed in the nodules of the Pouch of Douglas or the rectum. No other major tumorous lesions apart from the omental mass were found, suggesting that the YST had arisen from the omentum. Serum AFP levels returned to normal after surgery. Four weeks after secondary cytoreductive surgery, the woman underwent the BEP regimen combination chemotherapy again for one cycle. After one cycle of chemotherapy, she had chest pain. Electrocardiography, echocardiography, and chest radiography were performed, but there were no significant changes. She wanted to stop the chemotherapy, so it was ceased. Recurrence after completion of the chemotherapy has not occurred for 10 months.

Discussion
This is a case of extragonadal YST arising in the omentum. The histogenesis of YST of the omentum remains unclear. Several hypotheses have been suggested. One hypothesis is that the tumor originates from primordial germ cells that have been misplaced during embryonic migration. 2
Primary YST of the omentum in females is very rare, and this is only the fifth case to be reported in the literature.2,3 In the previously reported literature, the four patients received primary surgery and adjuvant chemotherapy. In this case, we performed exploratory laparotomy for primary surgery, which resulted in resection of only a small volume of the tumor, which was diagnosed as YST, and the woman underwent four cycles of BEP chemotherapy. After the chemotherapy, we performed secondary cytoreductive surgery and completely removed the residual tumor.
Cisplatin-based combination chemotherapy regimens such as BEP have improved survival rates for germ cell tumors, including YST, 4 and recently, BEP regimens have been established as an effective treatment for YST, with complete remission and cure rates of 80%–90%. 5 The chance of complete recovery now approaches 100% for early-stage patients and at least 75% for more advanced-stage patients. 6 Three courses of BEP is the current standard postoperative adjuvant chemotherapy regimen for female patients with YST with no or small-volume residual tumor after primary surgery, and four courses of BEP is recommended in cases of bulky residual disease after surgery. 7 In our case, optimal cytoreductive surgery was not achieved to avoid adjacent organ injury, so we administered BEP regimen chemotherapy for four cycles. In the previous literature, one case reported a successful treatment outcome that consisted primarily of chemotherapy and secondary cytoreductive surgery. 8 Chemotherapy using cyclophosphamide, cisplatin, and doxorubicin was administered. Serum AFP levels decreased to normal after surgery. YST usually responds well to cisplatin-based combination chemotherapy, such as the BEP regimen. Thus a treatment strategy that includes chemotherapy before surgery could be considered if optimal cytoreductive surgery could not be achieved.
The value of a second-look operation is not established for patients with YST. 6 It is reasonable to omit surgery in patients whose AFP levels return to normal. 9 In our case, after four cycles of BEP therapy, there was an 8-cm diameter residual tumor and the AFP level was 48 ng/mL. There was no evidence confirming whether similar chemotherapy should be continued or secondary cytoreductive surgery should be performed in this situation. Chemotherapy might be effective, but bleomycin induces toxicity, and clinically significant pulmonary fibrosis may occur if chemotherapy is continued for many cycles. To avoid bleomycin-induced lung toxicity, cisplatin-based chemotherapy excluding bleomycin such as combination of etoposide and cisplatin (EP) may be considered. But chemotherapy that omits bleomycin also may result in a poor outcome. 10 Bleomycin is one of the key drugs used in chemotherapy for YST. So we thought that we should use chemotherapy that included bleomycin. In epithelial ovarian cancer, which is sensitive to chemotherapy, optimum surgical debulking to leave residual tumor deposits that are <1 cm in size is associated with improved patient outcomes. 11 We employed the treatment strategy used for epithelial ovarian cancer. We thought that secondary cytoreductive surgery of the tumor might be effective. Residual tumor size strongly influences prognosis, 7 and for patients who already have children and do not wish to preserve their fertility, it seems reasonable to perform complete excision of all visible residual tumor and a bilateral salpingo-oophorectomy and total abdominal hysterectomy.4,7 There were no viable tumor cells in the resected tumor specimen. We were able to get rid of the residual tumor completely with surgery. After the secondary cytoreductive surgery, we planned to continue chemotherapy for several cycles for the purpose of consolidation chemotherapy. This is because there is no established protocol recommending adjuvant chemotherapy in extragonadal cases of YSTs when complete pathological remission is achieved. In this case, the patient underwent only one cycle of BEP regimen chemotherapy, and no recurrence occurred.
Serum AFP is a useful marker for diagnosis, monitoring the effectiveness of treatment, and detection of recurrence in patients with YST. 12 Our patient is followed up every month with a physical examination and serum AFP level testing. She has remained disease free for 10 months after completion of therapy. In conclusion, this is the first case report representing primary omental YST in a 34-year-old female treated successfully with prior BEP combination chemotherapy and secondary cytoreductive surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.