
Abstract
Abstract
Introduction
Loop stoma is preferable to end stomas for patients with poor performance status because they require smaller surgical incisions, and laparoscopy may be adequate. 7 However, higher rates of stomal complications including incomplete fecal diversion, retraction, and prolapse are described with the loop stoma. 8 Our standard surgical approach was to fashion the loop stoma over a glass or plastic bridge/rod,9–11 and we found that elevation of the shortened mesentery sometimes necessitated use of a pliable rubber tubing (red rubber catheter) instead. The bridge was left in situ for 7–10 days while the initial mucocutaneous healing took place. During this time, stoma care was made difficult by the need to fit the appliance under the projecting ends of the bridge, and this delayed patient self-care. Sometimes removal of the rod was followed by retraction and infection. 12 Stomal complications lead to a delay in chemotherapy or radiotherapy for patients planning active treatment and failure to achieve discharge to home/hospice care for others in a terminal palliative care framework. Jarpa 13 previously described a skin bridge technique for colostomy. We adopted this technique and also applied it to enterostomies. We audited our practice prospectively to assess its suitability for patients in a gynecological cancer center. The procedures were undertaken by specialist gynecological oncologists between October 2010 and February 2012 in a gynecological cancer center that cares for 300 new cancers per annum.
Criteria for surgical intervention and measures of success in relieving bowel obstruction have been addressed by others in an attempt to aid the clinician in selecting patients for surgical intervention.3,14 Arbitrary survival and palliative intervals have been recommended. 15 We considered it best to rate individual outcomes based on the patients' individual clinical circumstance and goals. Patients were considered to have achieved their immediate surgical goal if they were self-caring for the stoma and progressed to their planned further treatment (chemotherapy or radiation) and if they were discharged from hospital. Subsequent complications and survival were noted.
Surgical Technique
Patients are seen and marked by a stoma therapist prior to transfer to the operating theater. Once the patient is cleaned and draped, the stoma sites are re-marked with a sterile pen. For laparotomy, a small midline incision is made. The Hassan (cut-down) technique is used for laparoscopic entry. The intestine is surveyed to select the segment of bowel to be mobilized, and then the selected pre-marked stoma site is prepared for loop colostomy/ileostomy. The skin is dissected to create a central narrow (4–7 mm) skin bridge. The two D-shaped pieces of skin on either side of the bridge are discarded. The skin bridge is divided to create two skin flaps of unequal length. These skin flaps are dissected free of the rectus sheath with the subcutaneous tissue attached. Dissection is carried downwards through the rectus sheath and peritoneum, and the intestinal loop is delivered through the stoma using a nylon tape run through a fenestration in the mesentery of the bowel. The longer skin flap is pulled through this fenestration. The subcutaneous aspects of the skin flaps are opposed by holding the ends with Allis tissue forceps and sutured together with a monofilament non-absorbable 2-0 suture (Figs. 1–3). The suture can be placed at any level along the skin flaps to vary the tension of the bridge. When the permanent skin bridge is secured, the laparotomy/laparoscopy wounds are closed and covered with occlusive dressing before the bowel lumen is entered. The stoma is matured with interrupted mucocutaneous sutures with monofilament absorbable 3-0 sutures (Fig. 4). The condition of the stoma and the patients' progress towards self-care were recorded by the stoma nurse/therapist on a daily basis.

Two D-shaped skin pieces are excised, leaving a skin bridge.
The skin bridge is cut to give a long and short segment.

The longer segment of skin bridge is pulled through the fenestration in the mesentery.

Loop ileostomy following mucocutaneous suturing with 3-0 monofilament.
Results
Between October 2010 and February 2012, 16 patients had loop stomas fashioned in independent procedures for the treatment of small bowel obstruction (4), large bowel obstruction (5), multifocal obstruction (1) anastomotic leakage (1), sigmoid perforation (1), fistula (2), sigmoidoproctitis (1), and locally advanced vulvar cancer (1).
Nine patients had ovarian cancer—eight had recurrent disease and one patient developed bowel obstruction during primary chemotherapy for ovarian cancer. Four patients had cervical cancer—one at presentation at imminent risk of rectal fistulization; one proctosigmoiditis following chemo-radiotherapy for Stage IIIB disease; one Stage IIIB developed sepsis, large bowel obstruction with malignant perforation of the uterine fundus on the 5th day of external beam primary radiotherapy; and one recurrent adenocarcinoma of cervix with incomplete rectosigmoid obstruction starting palliative chemotherapy. The patient with vulvar cancer had disease abutting the anus. Two patients with suspected malignancy had diverticular disease with perforation/fistulization and pelvic sepsis.
The cancer patients ranged in age from 36 to 89 (median 58) years. All were bed ridden with the exception of the cervical cancer patient with imminent fistulization. Their anesthetic assessments were graded using the American College of Anesthesiologists (ASA) scale as grade 2 (10), grade 3 (4), or grade 4 (2). All patients had CT imaging preoperatively. The patients with bowel obstruction had nasogastric suctioning for between 1 and 18 (median 7) days. Two patients with large volume malignancy became acutely septic with the onset of bowel obstruction: one with clinical Stage IIIB cervical cancer in the first week of radiotherapy (patient X) and another with bulky Stage IV carcinosarcoma of the ovary who had received her first cycle of carboplatin/paclitaxel 7 days prior (patient Y). Patient X had malignant perforation of the uterine fundus and complete obstruction of rectosigmoid. Patient Y had multifocal small and large bowel obstruction secondary to large volume intra and retroperitoneal metastasis. All procedures were performed under general anesthetic. Two cervical cancer patients had laparoscopy, and all others had open laparotomy. The laparotomy was midline and limited to 10 cm or less in 12 patients. Two patients had more extensive exploration dictated by the extent of their multifocal obstruction and adhesions. The stoma was fashioned from the jejunum (1), ileum (9), and colon (6). One patient (patient Y) had jejunostomy and sustained two enterotomies in the attempt to expose the ileum.
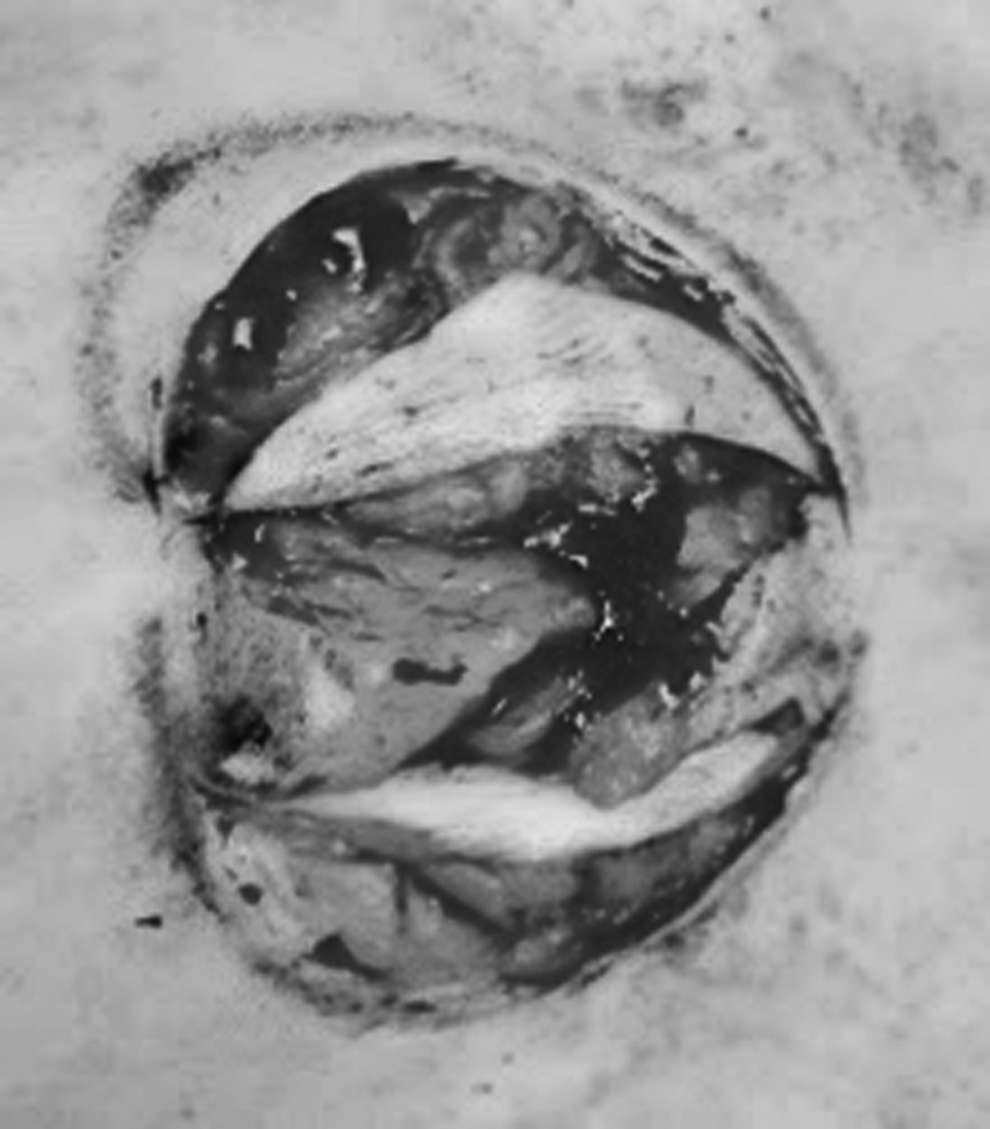
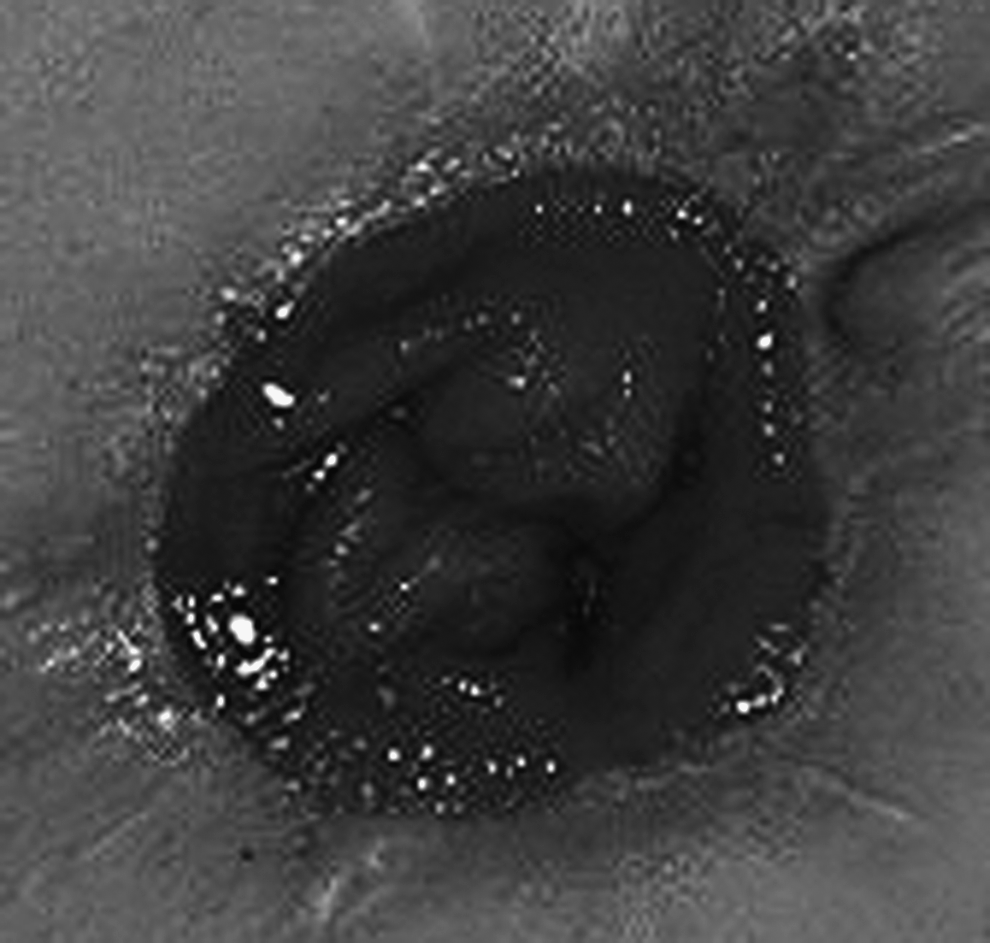
Patients X and Y remained septic and died 2 and 6 days respectively following surgery. All other patients recovered and were tolerating a low residue diet prior to discharge from hospital 4–12 days postoperatively. Cleaning and application of the stoma appliance were easy, and patient training was started on the second postoperatively day for 12 patients. Two patients who underwent laparoscopic assisted stoma formation started their stoma care training within 24 hours of surgery. Patients were competent in stoma self-care within 2–8 (median 5) days. The stoma pouted satisfactorily in all patients, and there were no stoma related complications. All except one patient with high output stoma discontinued TPN and intravenous fluid support, and all were tolerating low residue diet within 5 days of surgery. Six patients—five ovarian cancer and one recurrent adenocarcinoma of cervix—progressed to chemotherapy. Chemotherapy commenced within 20–38 (median 24) days of surgery. One patient with cervical cancer started her scheduled chemo/radiotherapy on postoperative day 16. The patient with advanced vulvar cancer had radical excision, including partial excision of the anal canal, and achieved negative histological margins. Fourteen patients were discharged home or to hospice care. Six patients died of progressive disease 6 to 30 weeks after surgery. No stomal complications arose in 6–73 weeks after bowel diversion. The outcomes were cosmetically satisfactory (Figs. 5 and 6). None of our patients had their stoma reversed.
Skin bridge loop colostomy at 110 days.

Skin bridge loop ileostomy at 84 days.
Discussion
Defunctioning enteral or colonic stoma is an integral part of the gynecological oncologist's surgical role. We had found the traditional plastic rod or rubber catheter support unsatisfactory for some patients due to stomal complications and delayed self-care, and we changed our practice to a skin bridge support of the bowel loop with satisfactory outcomes. The delay in starting self-care was eliminated, and the patients started self-care as early as the first postoperative day. Cleaning of the mucocutaneous wound and application of the plate/phalange for the stoma bag were easy. Previously described complications of necrosis, infection, retraction, and bypassing of fecal stream8,16,17 were not seen in our cohort up to 72 weeks of follow-up.
Our skin bridge loop technique is based on the colostomy described by Jarpa in 1986, 13 and we applied it successfully to ileostomy as well. The skin bridge would be expected to shorten with fibrosis following healing, and this results in good elevation of the bowel loop above the surrounding skin. The fibrosed permanent skin bridge is strong enough to resist retraction, even in ovarian cancer patients in whom shortening of the bowel mesentery by subsequent disease progression sometimes results in late retraction of the stoma following removal of a temporary bridge support.
Overall survival reflects disease progression in patients with very advanced gynecological malignancy.15,18–20 The two patients (12.5%) who died within a week of their surgery had sepsis at the outset. All other patients achieved their immediate surgical goals of discontinuation of nasogastric suctioning, progression to intervention therapy, and/or discharge to the appropriate palliative care setting. While none of our patients were candidates for reversal, take down of a skin bridge stoma could be performed in a standard fashion by incising around the circumference, mobilizing the loop, trimming back the mucocutaneous edge, closure, and return to the peritoneal cavity.
The decision to intervene surgically is complex in these very ill patients2,3,5,14 and has to be individualized to the patients' needs and wishes. The good postoperative performance with this skin bridge technique is encouraging, and we recommend its application to loop ileostomy and colostomy in gynecological cancer patients.
Footnotes
Disclosure Statement
No competing financial interests exist.