
Abstract
Abstract
Introduction
Case
A 16-year-old mentally subnormal girl presented to the gynecology outpatient department with amenorrhea of 2 years' duration. She also had a history of a lump and pain in the abdomen. Her mother reported poor weight gain in the previous few months and occasional attacks of vomiting after eating. On examination, the young girl was found to be anemic, with koilonychia and low body mass index (17kg/cm2). Abdominal examination revealed a nontender, firm, mobile large mass occupying the epigastrium and extending to her right hypochondrium and right lumbar region. The rest of the findings of the systemic examination were normal. The patient was admitted for detailed evaluation. Laboratory tests revealed hemoglobin: 7.2 g%; and mean corpuscular volume (MCV): 54.4 fL, consistent with microcytic hypochromic anemia. Blood, urea, serum electrolytes, urine examination, liver function test results, and thyroid function test results were within normal limits. A plain radiograph of the girl's abdomen showed a prominent gastric outline. Ultrasound of the abdomen revealed a large intragastric mass with acoustic shadows. Therefore, the patient was referred to the gastroenterology department. A barium meal study and computed tomography (CT) scan showed a large solid mass in a distended stomach (Figs. 1 and 2). The mass filled the entire stomach from the fundus to the antrum. The patient underwent endoscopy, which confirmed the presence of a large trichobezoar in the stomach extending from the cardia to the antrum (Fig. 3). There was a shallow ulcer on the gastric antrum with no extension of the bezoar into the duodenum. A more-detailed evaluation confirmed a history of hair ingestion. The patient's guardians did not give consent for surgical intervention.

Computed tomography (CT) film showing a large trichobezoar occupying the whole of the stomach.
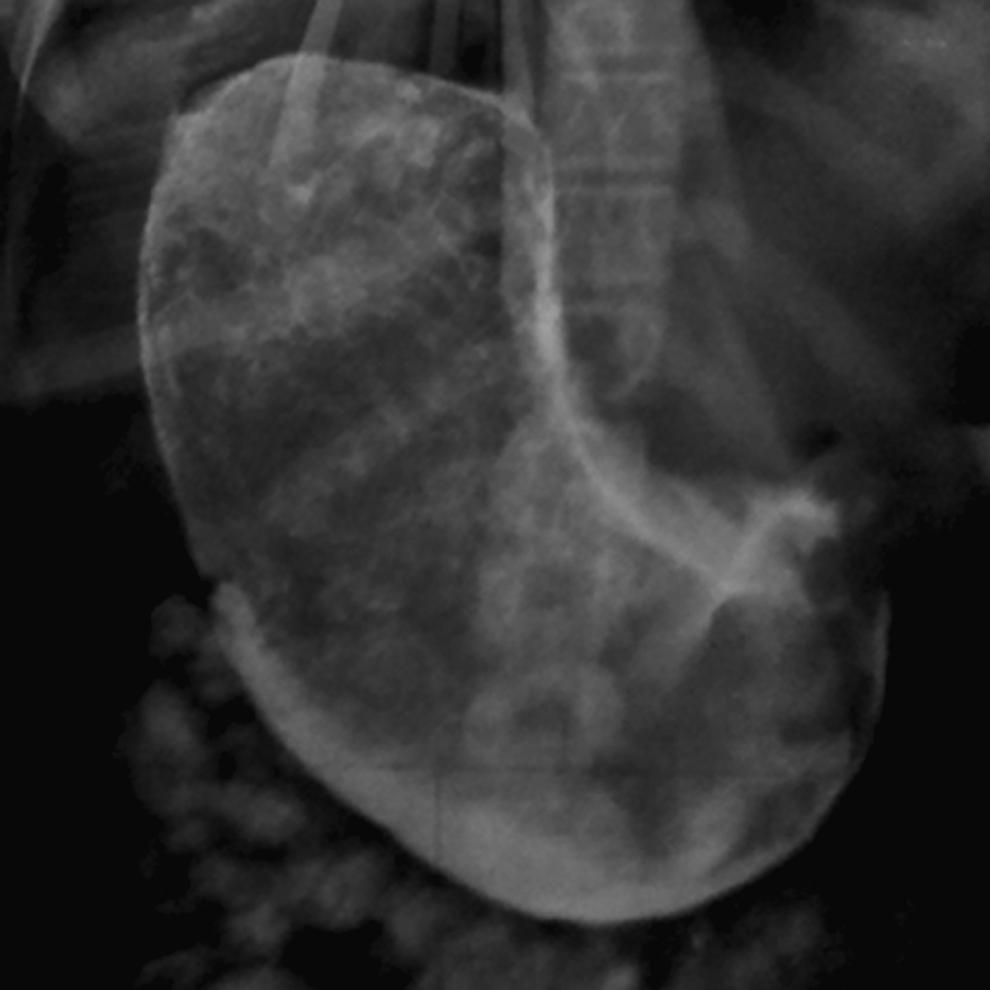
Barium meal showing a large trichobezoar.
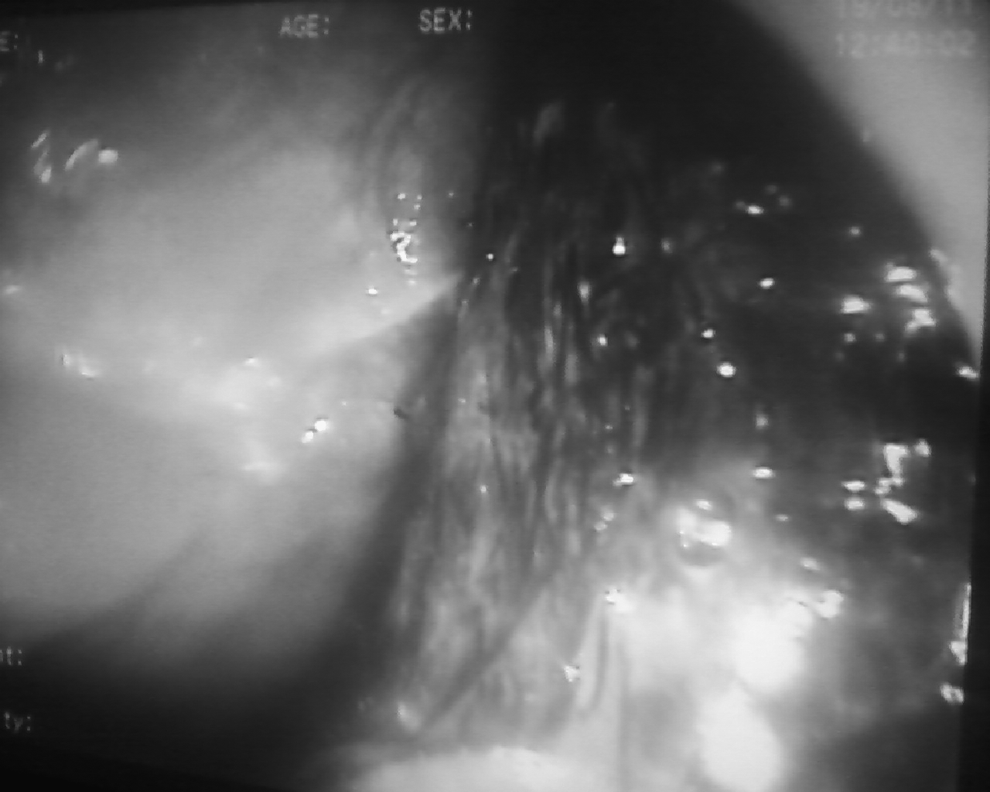
Endoscopic view of trichobezoar in stomach.
Results
The trichobezoar was too large to be removed in one piece; therefore, it was removed in multiple sittings using an endoscope (Fig. 4). The patient was referred to a psychiatrist for long-term management.

Endoscopically removed trichobezoar.
Discussion
Trichobezoars are GI masses formed from the accumulation of ingested hair. They grow slowly over many years and form a cast in the shape of the stomach and sometimes extend to the small bowel. DeBakey and Ochsner reviewed 172 cases of trichobezoar of which 90% were females in the 10–19-year age group. 3 Trichobezoars are generally seen in emotionally disturbed patients. 4 The hairs swallowed are trapped in the gastric mucosal folds and become enmeshed because of insufficient friction necessary for forward propulsion by peristalsis. The ingested hairs always become black because of the denaturation of hair proteins by the gastric acid. The patient reported here was a 16-year-old emotionally disturbed girl.
The symptoms of gastric trichobezoar depend upon its stage of formation and the length of time it is present. Usually, there are no symptoms until the trichobezoar reaches substantial size; a trichobezoar of 2500 g has been reported. In the beginning, the symptoms are vague and nonspecific, and develop gradually. 3 The usual symptoms are epigastric pain, nausea, vomiting, weight loss, anemia, diarrhea, or constipation. A large firm mass may be palpable in the epigastrium. The continuous growth of trichobezoars can cause pressure necrosis with resultant mucosal erosions and ulcerations, found most commonly along the lesser curvature, and have been reported in 10% of the patients. 4 Subphrenic abscess formation has been described in only 2 cases. The gastric trichobezoar and its tail may rarely extend through the entire length of the small intestine, the so-called “Rapunzel syndrome,” which was first described by Vaughan et al. in 1968. 5 Iron-deficiency anemia is the most common laboratory finding. 6 In this patient, secondary amenorrhea was the presenting symptom, and could have been the result of her iron deficiency anemia. Pain and a lump in her abdomen were also present.
The final diagnosis is based on a careful history, a thorough physical examination, and radiologic evidence. On examination, the features to look for are alopecia circumscripta, and a mobile abdominal mass in the epigastrium. If there are signs of obstruction, this will usually be in the small bowel, although colonic obstruction has been reported. Sometimes, a trichobezoar causes intermittent gastric outlet obstruction. The mass may be identifiable on palpation via a physical sign introduced by Lamerton. 7 Some of these signs can lead to suspicion of malignant disease. Plain films of the abdomen are of limited use, apart from confirming a clinical diagnosis of obstruction. Sometimes, a plain film of the left upper quadrant will show a mass in the stomach, which a barium meal will show to be a near-perfect cast of the stomach. Barium studies are of maximum benefit in the small bowel, in differentiating obstruction caused by adhesions from obstruction caused by bezoars. The typical CT image of a gastric trichobezoar is a well- defined ovoid intraluminal heterogeneous mass with interspersed gas. 8 If the trichobezoar is distal to the stomach and causing an obstruction, there will be dilated intestinal loops in addition to the intraluminal mass with gas retained in its interstices. Beyond the lesion, the bowel collapses. In Rapunzel syndrome, CT scans have shown a hypodense lesion in the stomach with a meshlike pattern. Oral contrast is sparse within the mesh, although the contrast is prominent around the margins. The presence of a tail is reflected by small rounded areas of hypodensity in other parts of the small bowel. Magnetic resonance imaging seems to be less useful than CT for diagnosis of trichobezoar, because the signal density is low and easily confused with air. 9 Sonographic features are not pathognomic. In this patient, diagnosis of trichobezoar was possible with a barium meal, ultrasound, and CT. Final diagnosis was made with endoscopy. Ko et al. noted that an arclike surface echo casting a clear posterior acoustic shadow within the dilated lumen can suggest the diagnosis. 10 Malpani et al. reported 3 patients, each with an with epigastric mass, in whom the diagnosis was not suspected clinically. Sonography each of the 3 patients revealed a hypoechoic curvilinear dense strip at the anterior margin of the lesion associated with acoustic shadowing and no through transmission. The diagnosis was confirmed by a barium meal and surgery. 11
A large trichobezoar has been conventionally removed by laparotomy, which has entailed an upper abdominal incision. With the advent of laparoscopic surgery, it became feasible to retrieve a foreign body from the stomach without the necessity of a laparotomy. As the majority of the patients are young females, cosmesis becomes more important in this situation. Endoscopic removal is usually not successful and results only in the retrieval of a small portion of the gastric trichobezoar. However, Wai et al. have reported that endoscopic retrieval is possible and open surgical or laparoscopic gastrostomy may be tried only if this fails. 12 Many endoscopic techniques have been described for breaking the trichobezoar up. These include use of instruments, such as normal biopsy forceps, polypectomy snares, foreign body forceps, endoscopic injection with enzymes, water-jet spray, and a lithotripter. In this patient, the trichobezoar was be removed with endoscopy in multiple sittings.
Conclusions
Counseling by a psychiatrist has an important role in prevention of recurrence. Trichobezoars should be considered a differential diagnosis in any young girl who presents with epigastric pain, vomiting, and an abdominal mass.
Footnotes
Disclosure Statement
No competing financial interests exist.