
Abstract
Abstract
Introduction
Case
A 52-year-old woman presented with complaints of abdominal pain of 1 month's duration and a single episode of postmenopausal bleeding 15 days prior. Findings from the general physical examination were normal, and a pelvic examination revealed bilateral ovarian masses 10×10 cm in size, solid in consistency, mobile, nontender, and with irregular margin. A pelvic sonogram suggested that ovarian masses were malignant. All other abdominal organs were normal on ultrasound. CA-125 was 945 international units (IU)/mL. Computed tomography

Bilateral Krukenberg tumor of the ovary.
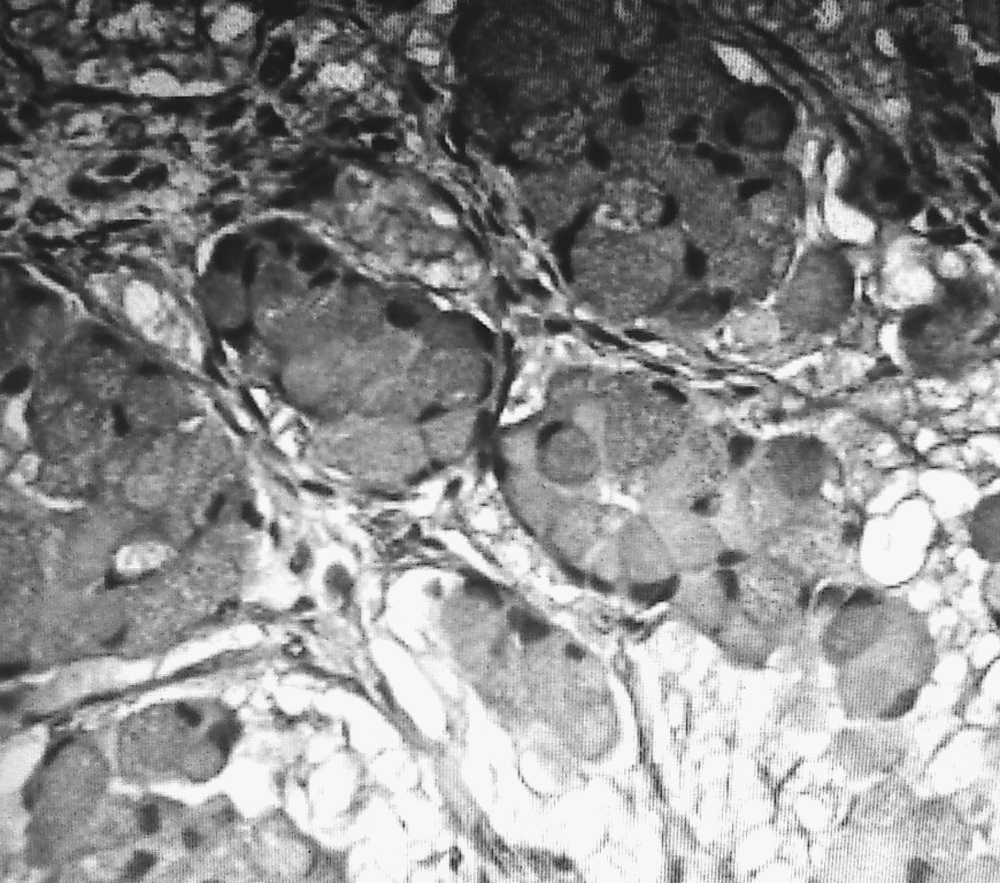
Microscopic examination of the sections from ovaries showing mucin-laden signet ring cells, within a cellular ovarian stroma.
Results
The patient is well and without any recurrence at 18 month follow- up.
Discussion
Krukenberg tumor is a rare metastatic signet ring-cell adenocarcinoma of the ovary, accounting for 1%–2% of all ovarian tumors. Common presenting symptoms are abdominal pain and distension. The remaining patients have nonspecific gastrointestinal symptoms or are asymptomatic. In addition, Krukenberg tumor is reportedly associated with virilization resulting from hormone production by ovarian stroma. Ascites are present in 50% of the cases, and usually reveal malignant cells. 1
There are two main differential diagnoses of ovarian tumors with signet ring cells containing mucin. These are primary mucinous carcinoma and mucinous carcinoid tumors. Primary mucinous tumors of the ovary can contain cells with signet ring appearance at least focally. However, these tumors tend to be more commonly unilateral with a complex papillary pattern. Mucinous carcinoid tumors (either primary or metastatic, most commonly from the appendix) enter the differential diagnosis in this group by having cells that may assume signet ring appearance and resemble Krukenberg tumor cells. Although mucinous carcinoid cells stain with mucin stains similar to Krukenberg tumor cells, immunostains for chromogranin and synaptophysin are usually positive and can easily confirm the diagnosis in favor of mucinous carcinoid.1,3 Diagnosis of Krukenberg tumor with unknown primary warrants careful investigation, mainly of the digestive tract and other potential sites.
A history of a prior carcinoma of the stomach or any other organ can be obtained in only 20%–30% of the cases. 4 In many cases, the primary tumor is very small and can escape detection. In such a situation, diagnosis of Krukenberg tumor warrants careful radiographic and endoscopic exploration of the digestive system in an attempt to detect the primary carcinoma. In the present case, meticulous radiographic and endoscopic investigation failed to detect any primary carcinoma.
Novak and Woodruff
5
have defined the criteria to qualify a Krukenberg tumor as primary tumor of the ovary (primary Krukenberg tumor). This includes:
1. Complete postmortem examination if the patient was dead at the time of the case report. Absence of primary tumor in any organ except the ovary should be proved by a detailed autopsy study. 2. If the patient was living at the time of the case report, and a surgical resection of the tumor was performed, then the patient should have survived for ≥5 years. An analysis of 19 acceptable cases reported in the literature favor the existence of primary Krukenberg tumor of the ovary.
6
Conclusions
The prognosis of Krukenberg tumor is poor, and no curative treatment is currently available. 7 Distinction is of imminent importance, as classification of Krukenberg tumor as a primary ovarian tumor may lead to suboptimal treatment of the patient.
Footnotes
Disclosure Statement
No conflicting financial interests exist.