
Abstract
Abstract
Introduction
This article presents a rare case, in an adult patient, of multiple presacral ganglioneuromas, which, regarding the location, is the nineteenth case ever reported in the literature.
Case
A 31-year-old healthy woman underwent a routine gynecologic examination by transvaginal ultrasound, which, incidentally, revealed a mass in the pelvis. The patient did not report any back pain, weight loss, neurologic, or endocrinologic symptoms. Physical abdominal and neurologic examination was in normal range, but rectal examination confirmed the presence of a palpable pelvic mass just in front of the sacrum.
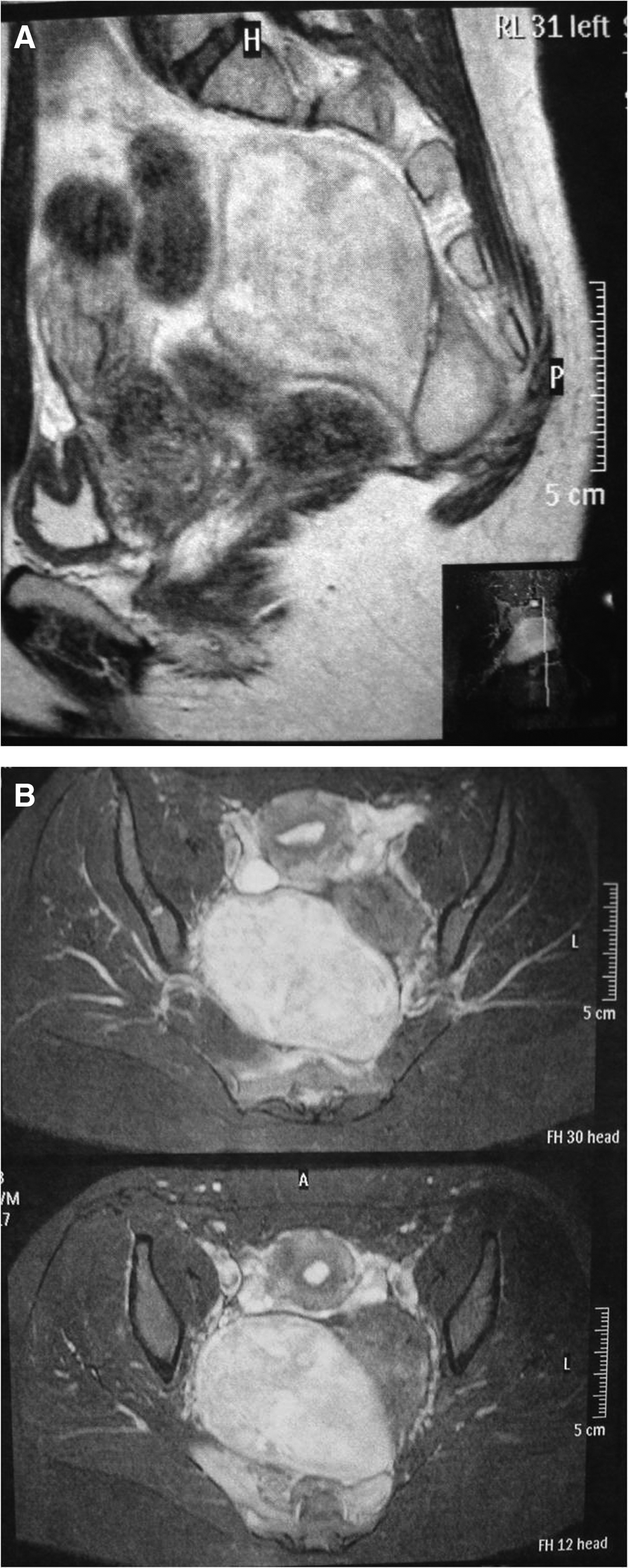
Laboratory studies, including complete blood cell counts, blood chemistry, and neoplastic markers (CEA, CA-15.3, CA-19.9, CA-125, α-fetoprotein, NSE, and CA CYFRA 21-1) were within normal limits. Sigmoidoscopy was negative for intraluminal infiltration. A magnetic resonance imaging scan (MRI) revealed the presence of three consecutive pelvic masses, with the largest measuring 10×10×0.8 cm, located in the presacral space, without infiltrating the adjacent structures (Fig. 1A, B).
The patient underwent laparotomy, and a complete resection of the three tumors was achieved. Intraoperative difficulties were associated with the tumors' large size, anatomical deep location, and origin from the presacral and coccyx area (Fig. 2A–C).
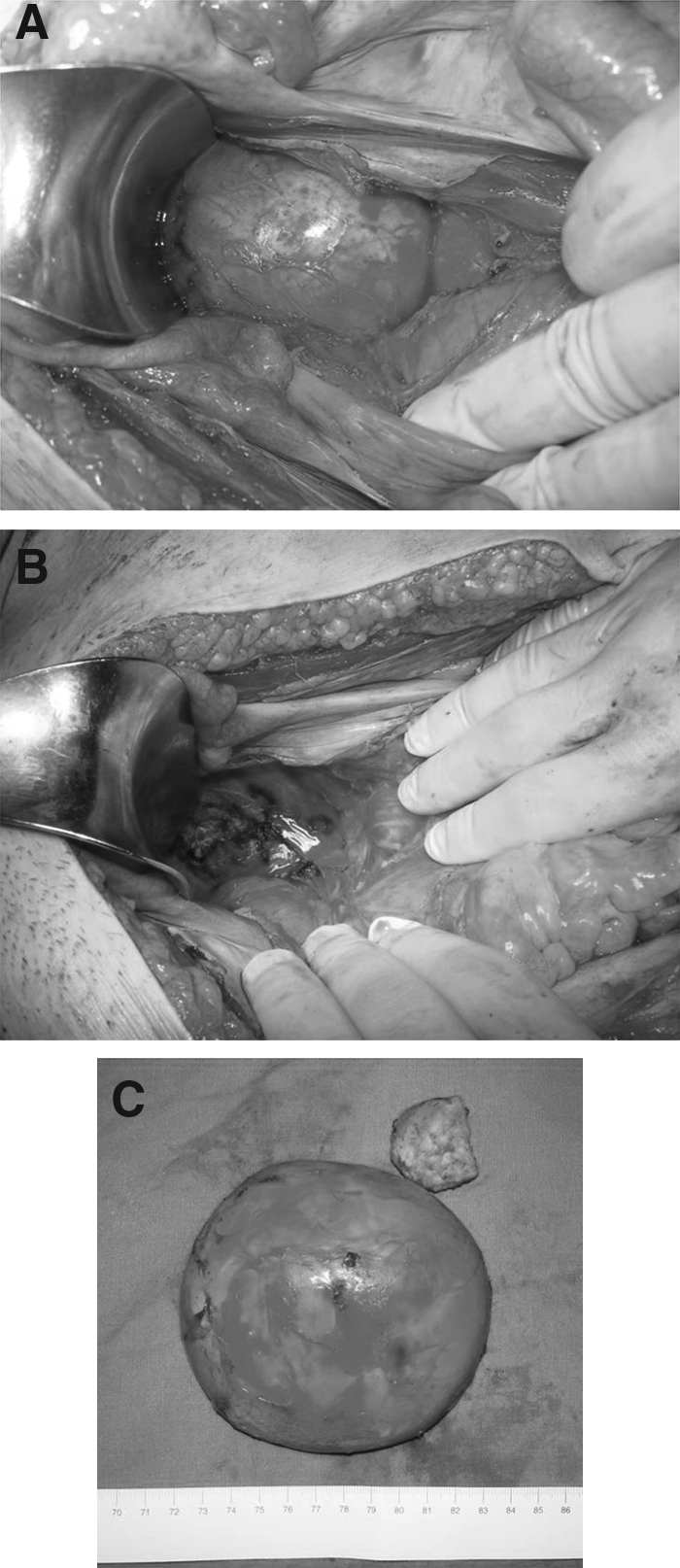
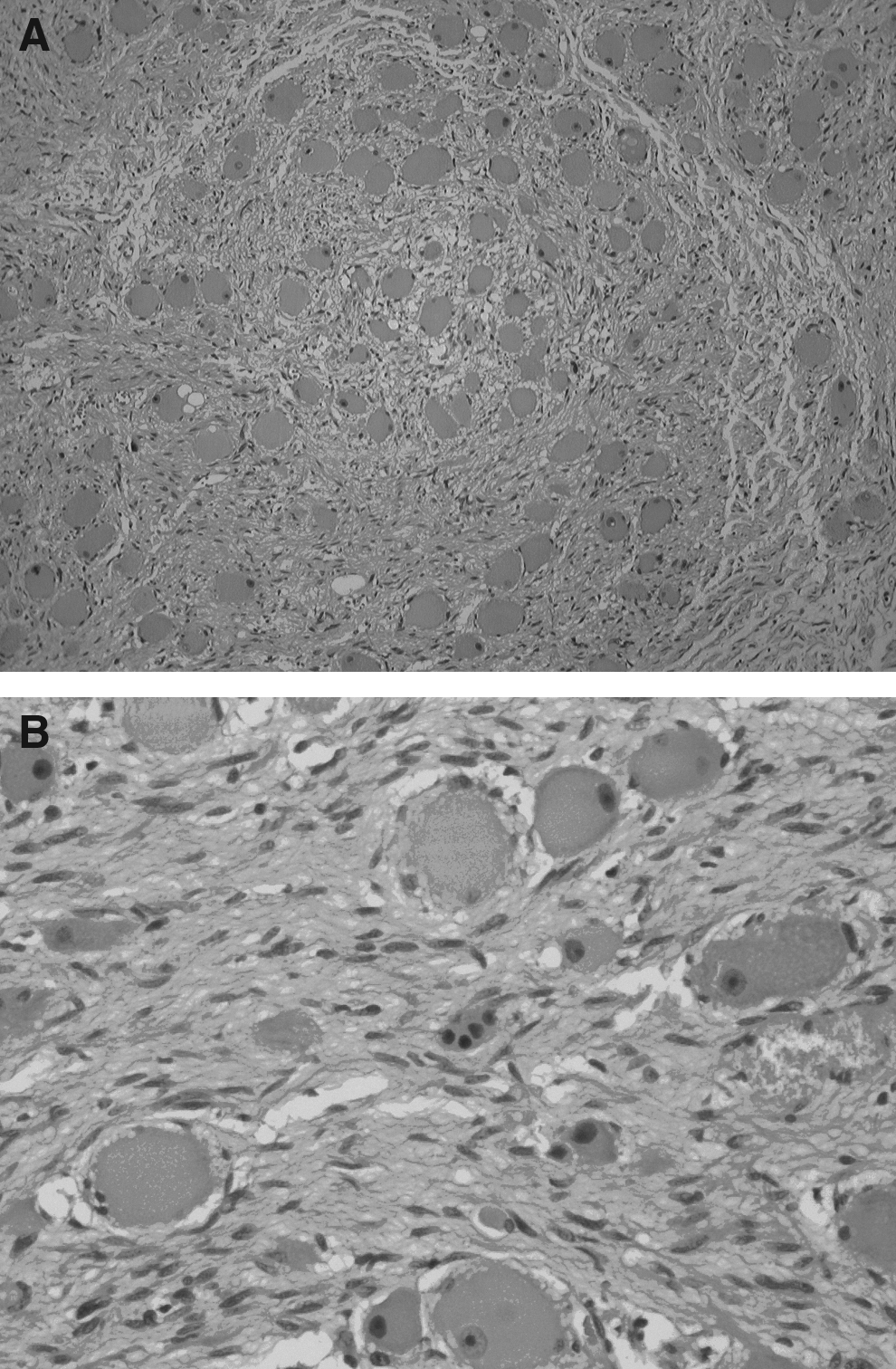
Frozen section revealed the benign nature of the tumors, identifying them as ganglioneuromas. Grossly, the tumors were 3.7 cm, 4.8 cm, and 11 cm in greatest dimension. They were encapsulated, of soft consistency, with a homogeneous white-to-yellowish cut surface. Microscopically, the tumors were surrounded by a thin layer of fibrous tissue and consisted of bundles of longitudinal and transversely oriented spindle cells, which crisscrossed each other in an irregular fashion. Mature ganglion cells having voluminous, bright eosinophilic cytoplasm with one or more nuclei, and sometimes prominent nucleoli, were found scattered or even in clusters or rests within the abovementioned spindle cell stroma (Fig. 3A, B). Pigment was present in some of the ganglion cells. Cellular atypia or mitotic activity was not observed. The above findings of pathologic examination were characteristic of ganglioneuroma without any evidence of malignancy. The diagnosis was also confirmed by immunohistochemical examination for S-100 protein, synaptophysin, neurofilaments, and Ki-67 antigen.
Results
The patient had an uneventful postoperative recovery and was discharged on the fifth postoperative day. During 6 months follow-up postoperatively, an abdominal MRI scan showed no recurrence.
Discussion
Ganglioneuroma is a rare, benign tumor of the autonomic nervous system and specifically of the sympathetic nerve system. 2 Ganglioneuromas may originate from regression and maturation of neuroblastoma cells, either spontaneously or following neuroblastoma treatment; or it may arise de novo.3,5,6 It consists of mature sympathetic ganglion cells, contrary to neuroblastoma, which is an immature cell tumor. 7 However, there are some reports of malignant transformation, spontaneously or after radiotherapy.8–11 Because of the fact that mature ganglion cells cannot multiply, ganglioneuroma is assumed to arise early in life.12,13 Therefore, it affects mostly young people, especially females, usually before the age of 20 in more than 60% of cases.14,15 In the current case, the patient was a 31-year-old woman.
Ganglioneuromas arise along the sympathetic chain usually as solitary tumors. Their most common location is the posterior mediastinum, lumbar retroperitoneum, pelvic retroperitoneum, adrenal medulla, and cervical spine, followed by paravertebral sympathetic ganglia, sympathetic paraganglia, bones, suprarenal space, and neck.1,2,7,16 A presacral location, as in the current case, is very rare and, according to the available literature, only 18 cases have been ever reported prior to this case.9,10,17–24 Moreover, this case seems to be the first report of multiple presacral ganglioneuromas, a condition quite unusual, which has been occasionally reported in patients with von Recklinghausen's disease.3,25 Ganglioneuroma has also been associated with multiple endocrine neoplasia syndrome Type II B. 14 The current patient had a medical history free of these clinical entities, which were also excluded from medical workup. Consequently, this case is rare for the number of tumors, their presacral site, the patient's age and the possible size of tumors, as the largest one of the three resected tumors measured 10×10×0.8 cm.
Similar to other benign neoplasms, the symptoms of ganglioneuromas usually occur as a result of enlargement of the tumor, leading to compression and displacement of the adjacent structures. The nature of the symptoms reflects the localization; as a result, patients with tumors of the presacral region may complain about constipation or pain caused by pressure on the rectum, sacral nerve roots, and lumbosacral plexus.7,15,26 The current patient was asymptomatic, which was also confirmed by physical and neurologic examination.
The differential diagnosis of presacral tumors is broad and includes schwannoma, neurofibroma, meningioma, cystic lesions, various lymphomas, chordomas teratomas, soft-tissue sarcomas, Ewing sarcoma, osteosarcomas, and chondrosarcomas. Therefore, such a case should be further evaluated by ultrasound, computed tomography (CT), or MRI, depending on the case. In an imaging scan, a ganglioneuroma typically shows punctate calcification and low attenuation on CT and marked hyperintensity on T2WI with gradually increasing enhancement on dynamic MRI.25,27 Among radiologic techniques, the MRI scan has the ability to provide important and determinant information, especially concerning tumor size, location, extent of tumor invasion, and the possible involvement of soft-tissue and neurologic structures.28,29 Moreover, it is the most suitable and reliable imaging method to provide characteristics and information helpful either in setting the differential diagnosis or preoperative surgical planes. Preoperative needle biopsy samples may be useful, but often the site of the tumor may not permit such an approach. 8
Nevertheless, the definite diagnosis is only made by pathologic examination. This is best accomplished by complete surgical resection of the tumor, which is the treatment of choice.3,25 The anterior laparotomic approach, transperitoneally, with rectum mobilization was chosen to achieve a complete and safe tumor resection, and to preserve nerve tissues. An alternative procedure—the posterior trans-sacral approach with sacrectomy—is reported to risk trauma in the dural sac and cauda equina, leading to possible permanent motor or sensory deficits or loss of bowel, bladder, or sexual function.30,31 Because of the benign nature of ganglioneuromas, adjuvant systemic chemotherapy or local radiotherapy are not indicated. 15 Because of a possible incomplete resection or the possibility of recurrence, annual follow-up with neurologic examination and pelvic MRI is required. Nevertheless, the recurrence rate for ganglioneuroma is near zero, and postoperative complications are rare.15,19
Conclusions
Multiple presacral ganglioneuromas are very rare, but they should be considered in the differential diagnosis of pelvic masses. Although these tumors are histologically benign, they may behave aggressively and/or compress adjacent structures. Given this potential, surgical excision remains the treatment of choice, also providing the definite diagnosis.
Footnotes
Disclosure Statement
No competing financial interests exist.