
Abstract
Abstract
Introduction
Case
A 23-year-old, gravida two, para one female, who was 5 months pregnant, was referred by a private practitioner to the obstetric department of the Postgraduate Institute of Medical Sciences, Rohtak, Haryana, India, for tertiary care in for an extrauterine pregnancy, which was diagnosed on routine ultrasonography. She had been married for 3.5 years, and had had a full-term normal vaginal delivery at home 1 year prior, and the child was alive and healthy. She had was no history of abortion. Her menstrual cycles were normal and regular, without any dysmenorrhea. There was no history of an antenatal checkup prior to this visit. She had complained of fluctuating mild pain for 3 months in her lower abdomen. She was prescribed pain killers for this, but the doctor who did so did not perform any examination of her condition. Her general condition was good, with a pulse rate 82 beats per minute, a blood pressure of 110/80 mm Hg, hemoglobin of 9.5 gm%, and an A-negative blood group. US at the Institute revealed a gestational sac with a fetus and placenta on the left side, with a biparietal diameter of 32 mm and a femur length of 19 mm, corresponding to 15 of weeks pregnancy; cardiac activity was present. The uterus was displaced to the right side; it measured 8.5×5.5 cm, with a normal echo pattern and contour. Both kidneys were normal in size and shape. Abdominal examination showed that her uterus was enlarged to the size of a 16-week pregnancy, deviated slightly to left, and was nontense and nontender. A vaginal examination revealed a uterus the size of a 16-weeks pregnancy that was deviated to the left, with no other masses felt separately.
Laparotomy was decided upon after explaining the diagnosis and management plans to the woman's relatives and arranging for an adequate blood supply preoperatively. The patient was also informed about the diagnosis and management plan. Operative findings revealed a 16-week-size pregnant rudimentary horn with the tube and ovary on the left side and attached to the right horn by a thick fibrous band of tissue (Fig. 1). The right horn of her uterus was enlarged to 8-weeks size with an attached tube and ovary. The rudimentary horn with the pregnancy in situ was excised along with the left tube (Fig. 2). Her left ovary was normal and was left in place. There was no need for a blood transfusion. She was given an injection of anti D and discharged on the third postoperative day, per her persistent requests, in good condition.
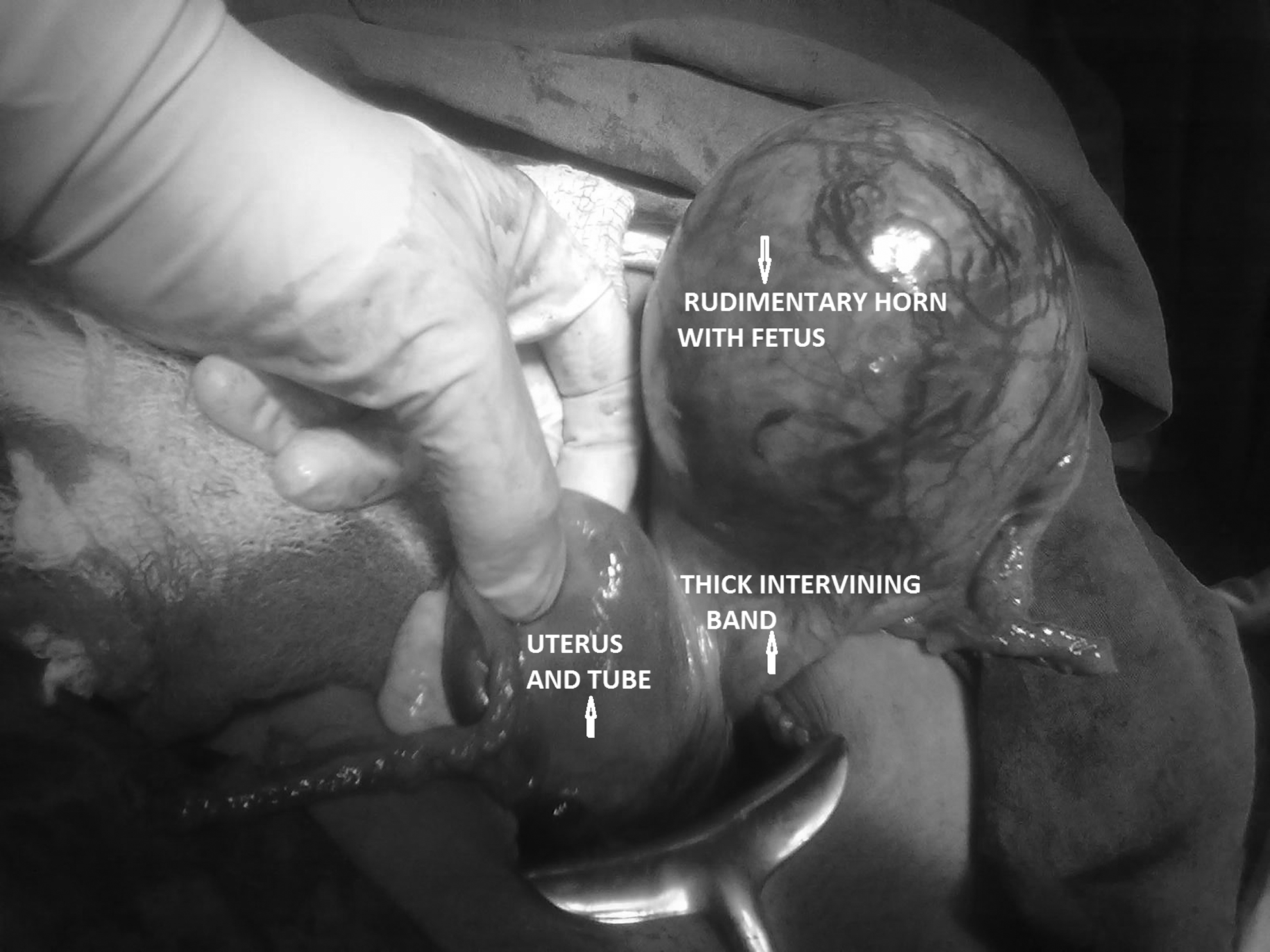
Unicornuate uterus with pregnant rudimentary horn attached by a fibrous band.

Excised rudimentary horn with placenta and fetus ensac.
Results
She returned for stitch removal on the eighth day and her postoperative period was uneventful. Hystopathologic examination revealed the structure of the rudimentary horn with the fetus and placenta in situ.
Discussion
A rudimentary uterine horn results from arrested development of the Müllerian ducts. It is a rare anomaly, and the incidence of rudimentary horn pregnancy is relatively less. From 1966 to 2003, only 156 cases of the pregnancy in a rudimentary horn have been reported.
8
Ninety percent of rudimentary horns are noncommunicating to the main uterine cavity, and pregnancy in the rudimentary horn results from transperitoneal migration of the sperm or conceptus.1,9 The majority of patients with Müllerian anomalies are asymptomatic. Dysmenorrhea (80%), urinary-tract anomalies (60%), hematometra, and endometriosis are commonly associated with the presence of a rudimentary uterine horn because of the existence of functioning endometrium.6,9,10 Prerupture diagnosis is difficult, but early diagnosis prior to rupture is essential for timely intervention and reduction of complications.
10
The condition is suspected clinically in the first trimester when manual palpation reveals a mass extending outside the uterine angle (Baart de la Faille's sign)
6
or displacement of fundus to the contralateral side with rotation of the uterus and elevation of the affected horn (Ruge Simon syndrome).
9
Three-dimensional US imaging and MRI are useful tools for improving diagnostic accuracy, patient counseling regarding the condition, and surgical planning.
11
Accuracy of US for diagnosis is fairly good at early gestation. As reported in the literature, there have even been reports of first-trimester prerupture diagnoses of rudimentary horn pregnancies, but only 5% of the reported cases were diagnosed preoperatively.4,12,13 In 1983, Holden and Hart reported the first case of prerupture US diagnosis of a rudimentary horn pregnancy.
5
Although it is difficult to distinguish accurately between a rudimentary uterine horn pregnancy and an interstitial pregnancy, it was reported that the main sonographic criterion for diagnosis of a rudimentary uterine horn pregnancy was an unusually thin uterine wall.
10
The following criteria have been suggested by Tsafri et al.1,12 for sonographic diagnosis of a rudimentary horn pregnancy:
(1) A pseudo pattern of an asymmetrical bicornuate uterus (2) Absent visual continuity between the cervical canal and the lumen of the pregnant horn (3) Presence of myometrial tissue surrounding the gestational sac.
Placement of a Foley's catheter into the uterine cavity prior to performing a transaabdominal US scan is obviously not a preferred method of diagnosing an extrauterine pregnancy but it has proven to be a useful and inexpensive way of excluding the possibility that a patient may have an intrauterine pregnancy. 1 As a result of underdevelopment and poor distensibility, pregnancy in a rudimentary horn terminates by rupture, missed abortion, or an intrauterine fetal death; rare fetal survival has been reported.4,8 The majority (70%–90%) of these pregnancies cause rupture before 20 weeks of gestation. Live births are rarely reported in patients with this condition. As noted in a review conducted from 1990 to 1999, only 6% of rudimentary horn pregnancies were reported to have progressed to term, with 13% neonatal survival, and this was because of earlier detection and intervention.5,8 Rupture of the horn is still common, but maternal morbidity and mortality rates have declined to ∼5% because of early intervention.1,10 When a rudimentary horn pregnancy is small, and facilities exist for managing it, it may be possible to resect it laparoscopically.8,12 Nahun has advocated conservative management, until viability is achieved in a few selected cases—if emergency surgery can be performed at any time and if the patient is well-informed. 14 Medical treatment with methotrexate for early pregnancy in a rudimentary horn and resection of such pregnancies via elective laparoscopy have also been reported. 15 The rudimentary horn should be excised, whenever the condition is diagnosed, to prevent a rupture in the pregnancy. 16
However, immediate surgery is recommended by most experts, and once the prerupture diagnosis of rudimentary horn pregnancy has been made, ideal management includes surgical resection of the horn along with the Fallopian tube on that side17–19 as was performed in the current case.
Conclusions
The incidence of rudimentary horn pregnancy is relatively small, and diagnosis prior to rupture is difficult. There is a need for increased awareness of this rare condition, and diagnosis of a rudimentary horn should be done before conception—or at least before rupture—to avoid fatality. US plays an important role in diagnosing rudimentary horn pregnancy. Thus, any patient complaining of lower abdominal pain in early pregnancy should be screened for this rare entity by US to reduce maternal and fetal morbidity, and, at times, mortality.
Footnotes
Disclosure Statement
None of the authors have a conflict of interest.