
Abstract
Abstract
Introduction
Primary amenorrhea can also be caused by anatomic defects of the müllerian system and can involve the fallopian tubes, uterus, cervix, and/or upper two thirds of the vagina. The prevalence of müllerian anomalies is 0.1%–3.8%.2,3 They can occur at any point in the female reproductive tract development process, leading to a wide spectrum of anatomic presentations. Absence of müllerian structures is referred to as “agenesis,” while underdevelopment is termed “hypoplasia.” Because vaginal and uterine agenesis and hypoplasia is a continuum, accurate diagnosis can be challenging. Since the ovaries develop independently from müllerian structures, women with müllerian anomalies usually have normal ovarian function and development of secondary sexual characteristics.
The combination of a hypogonadotropic hypogonadism and a müllerian anomaly is a rare cause of primary amenorrhea and makes diagnosis even more difficult. This article presents a patient with primary amenorrhea related to hypoplastic vagina, partial vaginal septum, and hypogonadotropic hypogonadism that was initially diagnosed as müllerian agenesis.
Case
A 34-year-old, nulliparous, white woman was referred for evaluation of primary amenorrhea and an inability to have coitus. She had been previously diagnosed as having müllerian agenesis at age 12 years. No records of previous evaluation of hormonal status or developmental Tanner staging were available. The patient did not report a lack of smell upon questioning or prior treatment with hormone therapy prior to breast development. Six months prior to referral, the patient had a transabdominal ultrasound scan that showed a hypoplastic uterus measuring 3×2×1.5 cm, 1 mm endometrial stripe, right ovary measuring 1.4×1.1 cm with no antral follicles, left ovary measuring 1.5×0.9 cm with no antral follicles, and no clear images of the cervix. An attempt at vaginal dilation was made at that time, which the patient was unable to tolerate. The patient was referred to the current authors' service for consultation because she was unable to be sexually active due to pain.
On clinical examination, the patient was obese with Tanner stage V hair development and breast development. Her external genitalia appeared normal. Her narrowed vagina was estrogenized, 1.5 cm in length, and appeared to end in a blind pouch.
Magnetic resonance imaging (MRI) revealed a hypoplastic uterus and vagina consistent with class I müllerian duct anomaly and normal kidneys, but the cervix was not clearly delineated. A two-dimensional transperineal and transrectal ultrasound scan showed a uterus measuring 2.5×1.7×0.6 mm, a 1-cm cervix, and a 2-cm decompressed vaginal opening just below the cervix.
The patient's karyotype was 46 XX, and her thyroid-stimulating hormone (TSH), testosterone, and prolactin were in the normal range. Her estradiol level was 18 pg/mL and follicle-stimulating hormone (FSH) was 0.9 IU/L. There was no evidence of a pituitary or hypothalamic abnormalities on MRI.
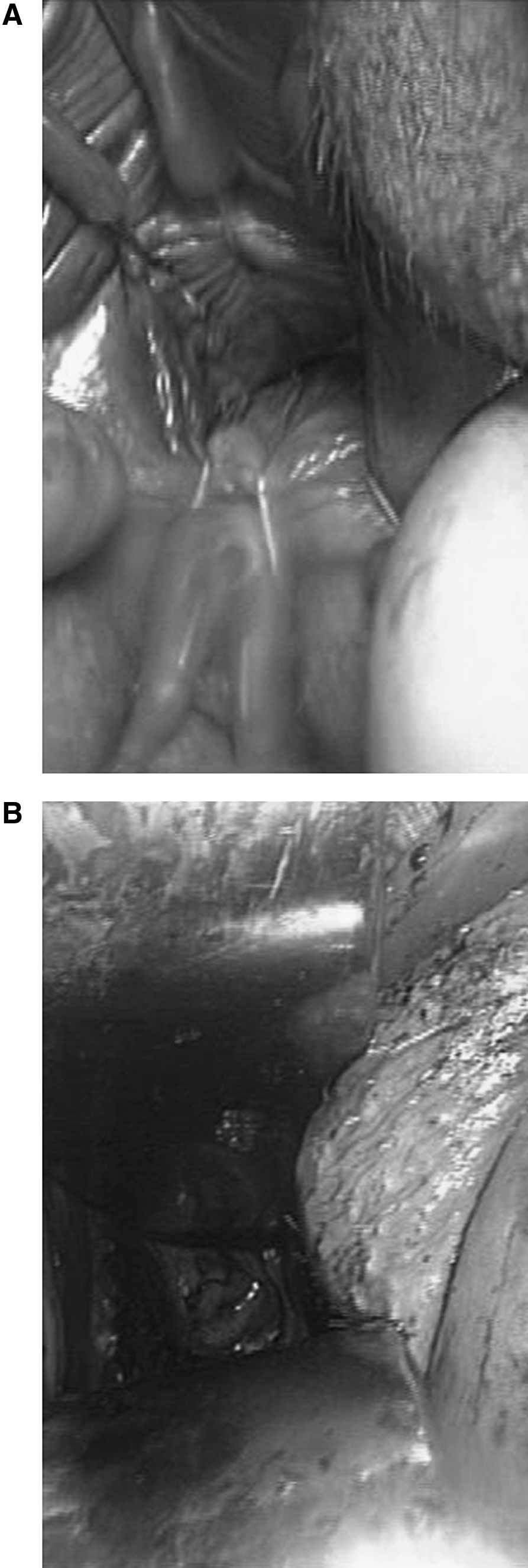
Diagnostic laparoscopy revealed a hypoplastic uterus, normal ovaries and tubes bilaterally, and no evidence of endometriosis or adhesions. Estimated sizes of the uterus and ovaries were consistent with measurements from the MRI and ultrasound scans. Vaginal examination with the patient under anesthesia confirmed a hypoplastic vagina ending in a blind pouch (Fig. 1A). On speculum examination, a pinpoint hole at the apex of the vagina was discovered, which was not originally seen during office examination. This small hole at the vaginal apex was opened into the upper vaginal cavity by gentle probing with Adson forceps, and a normal cervix was visualized (Fig. 1B). Once access was gained to the upper part of the vagina, the remaining partial vaginal septum at the level of the mid vagina was resected with a scalpel using a cruciate incision. At the conclusion of surgery, the vagina was 3 cm in diameter and 9 cm in length. An inflatable vaginal stent (Adjustable Vaginal Stent; Mentor® Corp., Minneapolis, MN) was inserted to maintain vaginal patency.
Results
The patient was discharged on the day of surgery and the vaginal stent was spontaneously expelled 2 days later. She was treated with transdermal estradiol (0.05 mg) patches replaced twice weekly, vaginal conjugated estrogen cream (0.5 g) weekly, and oral micronized progesterone (200 mg) 14 days per month. The patient was instructed to use vaginal dilators of increasing size as tolerated. Six weeks after surgery, she was able to use the medium dilator as well as have coitus with minimal to no discomfort. Three months postoperatively, her vagina appeared well estrogenized, and she began having monthly menstrual bleeding. Follow-up ultrasound scan to re-assess uterine and ovary size is planned 1 year after hormone therapy initiation. Currently, the patient is not seeking a pregnancy.
Discussion
A rare case is presented of a woman with primary amenorrhea secondary to hypogonadotropic hypogonadism combined with a hypoplastic vagina and uterus and partial vaginal septum. The only similar cases that could be found in the literature were a group of three families with the familial occurrence of primary hypogonadism with müllerian hypoplasia and partial alopecia.4–6 Prader–Willi syndrome can also present with obesity and hypogonadotropic hypogonadism, but the patient in the current report did not meet all clinical criteria for methylation studies, including a history of hypotonia, poor feeding in infancy, cognitive impairment, or hyperphagia. 7 Although the combination of hypogonadotropic hypogonadism, vaginal hypoplasia, and partial septum in this patient might be coincidental, this situation highlights the need for thorough evaluation of patients with primary amenorrhea. Careful laboratory and anatomic evaluation can prevent misdiagnosis of müllerian anomalies so that appropriate management can be initiated in a timely manner. 8
The evaluation of primary amenorrhea involves a combination of history, physical examination, laboratory tests, and imaging studies. History and physical examination are important for assessing development of secondary sexual characteristics and detecting cyclic symptoms suggestive of menstrual obstruction.
Laboratory evaluation of primary amenorrhea includes measurement of human chorionic gonadotropin, estradiol, FSH, TSH, prolactin, and total testosterone to diagnose the most common causes of amenorrhea and exclude androgen insensitivity syndrome. 8 Periodic re-evaluation of estradiol and FSH in women diagnosed with müllerian agenesis should be considered to prevent the effects of prolonged hypoestrogenemia, such as osteoporosis. 9
Exclusion of other causes of secondary hypogonadotropic hypogonadism should be considered if the patient has associated signs or symptoms of the disease. For example, a salivary or urinary cortisol and dexamethasone suppression test would have been obtained to rule out Cushing syndrome, or growth hormone and insulin-like growth factor-1 to rule out acromegaly.
Several gene mutations have been implicated in the pathogenesis of hypogonadotropic hypogonadism, including KAL-1 (Kallmann syndrome), GnRH receptor, HESX1, LHX3, PROP-1 (pituitary transcription factors), DAX-1, SF-1 (orphan nuclear receptors), and leptin receptor (gene associated with obesity). 10 These mutations were not evaluated because they were not readily available or covered by insurance. Suspicion was low for these genetic mutations since the patient in this report had already developed secondary sexual characteristics.
The initial imaging technique for the evaluation of müllerian anomalies continues to be ultrasound examination, although MRI may be reserved for complex cases. 8 At lease one report has suggested that three-dimensional ultrasound can also be an accurate method for diagnosing müllerian anomalies. 11 In the current case, a combination MRI and transperineal and transrectal ultrasound was used to confirm the presence of a uterus, cervix, and vagina, and to determine the location of the ovaries and kidneys. There was no evidence of hematometra or hematocolpos in this patient, which would have been anticipated if her only diagnosis was vaginal hypoplasia and septum resulting in outflow obstruction.
First-line treatment for vaginal agenesis and hypoplasia is mechanical dilation. Studies have shown up to 91% success with dilation of vaginal lengths less than 0.5 cm in both anatomic and functional areas for patients with agenesis. 12 Although the patient in this article did not have complete vaginal agenesis, dilation can benefit women with a hypoplastic vagina. 13
Once a diagnosis of midvaginal obstruction had been made, dilation is not an appropriate treatment option. In these cases, surgery is indicated to relieve outlet obstruction, and to provide adequate vaginal length sufficient to allow intercourse. The current patient appeared to have a partial vaginal septum, and connecting the lower and upper vaginal segments was easily accomplished with local excision. There is currently no consensus on the best surgical approach to vaginal hypoplasia.14 However, a combination of vaginal dilators and regular sexual activity can prevent postoperative stricture and help maintain healthy vaginal tissue.
Conclusions
In conclusion, evaluation of primary amenorrhea requires a combination of accurate laboratory and imaging techniques, particularly when pelvic examination is inconclusive. Hypoestrogenemia should be corrected to achieve normal secondary sexual development and to prevent osteoporosis. Müllerian anomalies should be thoroughly characterized. Menstrual outflow obstruction requires surgical treatment; vaginal hypoplasia can be treated with mechanical dilation and sexual activity.
Footnotes
Disclosure Statement
No competing financial interests exist.