
Abstract
Abstract
Introduction
Cotyledonoid dissecting leiomyoma (CDL; Sternberg tumor) was proposed as a new form of uterine leiomyoma with a benign histology but with a distinctive and alarming exophytic placental-like gross appearance extending from the uterus into the broad ligaments or the pelvic space. This benign smooth-muscle tumor with an unusual growth pattern may lead gynecologists and pathologists to a false diagnosis and patient overtreatment. For this reason, this variant of tumor, which can cause a diagnostic challenge, must be well known and kept in mind. We report herein four additional cases of this distinctive benign uterine tumor with unusual growth patterns and some histopathologic particularities.
Cases
Four cases of CDL were diagnosed in the pathology department of the Salah Azaiz Institute between 2006 and 2011. The clinicopathologic features of the four cases are summarized in Table 1.
TH, total hysterectomy; SH, subtotal hysterectomy; SO, salpingo-oophorectomy.
Case 4 was previously reported by us in 2008. 1 Patient ages ranged from 47 to 52 years (mean: 49.5 years). At laparotomy, three tumors extended from the wall of the uterine body; two of these tumors were located in the serosal side of the uterine fundus and were characterized by an extrauterine, exophytic, and invasive growth pattern. A multinodular cotyledonoid fungating appearance and extension from the uterine surface into the broad ligaments and the pelvic cavity were observed.
On gross examination, the tumors were soft to rubbery and varied from 7 to 30 cm in maximal diameter (mean: 18 cm). The cut surface showed a white (case 2) or deep red (cases 1, 3, and 4) multilobulated aspect (Fig. 1). The tumor described in case 3 had no intramural insertion and typically presented as numerous exophytic congested small nodules resembling placental cotyledons. An intraoperative frozen section was therefore unlikely to help in identifying the smooth-muscle origin of this tumor in cases 3 and 4.

The tumor formed deep red, multiple nodules wrapped by an anastomosing vascular network resembling placental cotyledons extending to the large ligaments.
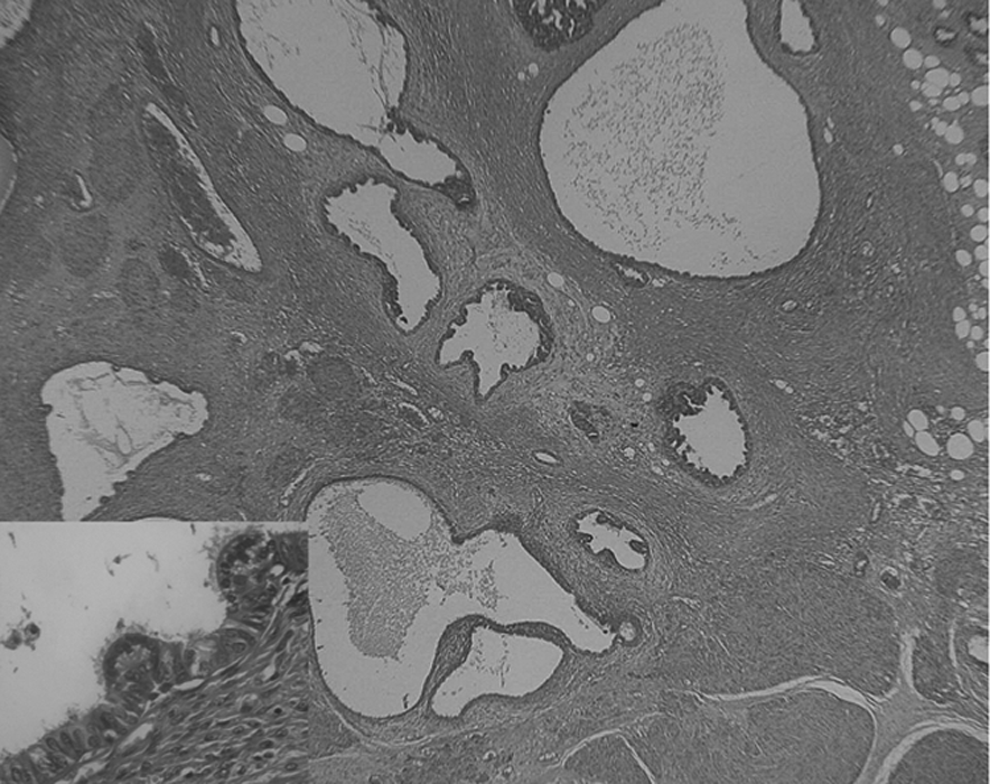
Histologically, the tumors in cases 1, 2 and 4 had two components: a cotyledonoid exophytic component and an intramural component. Both were predominantly formed of disorganized swirls of fascicules of smooth muscle demonstrating an irregularly dissecting growth pattern with elongated processes surrounded by hyaline fibrous matrix (Fig. 2). Nuclei were grossly regular with neither mitotic figures nor significant cytological atypia. Coagulative tumor necrosis was also absent. Small congested and dilated clustered veins were identified in interlobular regions. The tumor described in case 3 demonstrated only a cotyledonoid exophytic component with no evident histological mural dissection. An intravascular intrusion was found only in case 1. These tumors were accompanied by various histological benign lesions.

Multiple micronodules of smooth muscle dissecting the myometrium with a swirling growth pattern (inset), abundant congested blood vessels, and perinodularhydropic degeneration (inset). (H&E ×20; inset: H&E ×40.)
One case (case 4) demonstrated endosalpingiosis in the extrauterine cotyledonoid component, made of numerous glands and cysts lined with a ciliated tubal-type epithelium (Fig. 3). Another case (case 2) showed limited foci of endometriosis (Fig. 4).
Micronodules of smooth muscle within the myometrium adjacent to multiple limited foci of endosalpingiosis made of variously sized glands and cysts lined by benign-appearing epithelium in case 4 (H&E,×20). Inset: Lining epithelium showed a stratification of ciliated columnar cells (H&E,×40).

Smooth-muscle micronodules dissecting the myometrium with foci of endometriosis in case 2 (H&E,×10).
The tumor reported in case 3 displayed a cytological epithelioid pattern composed of sheets of epithelioid cells with finely granular, pale, eosinophilic cytoplasm and central bland nuclei with no nuclear atypia nor mitotic activity (Fig. 5).
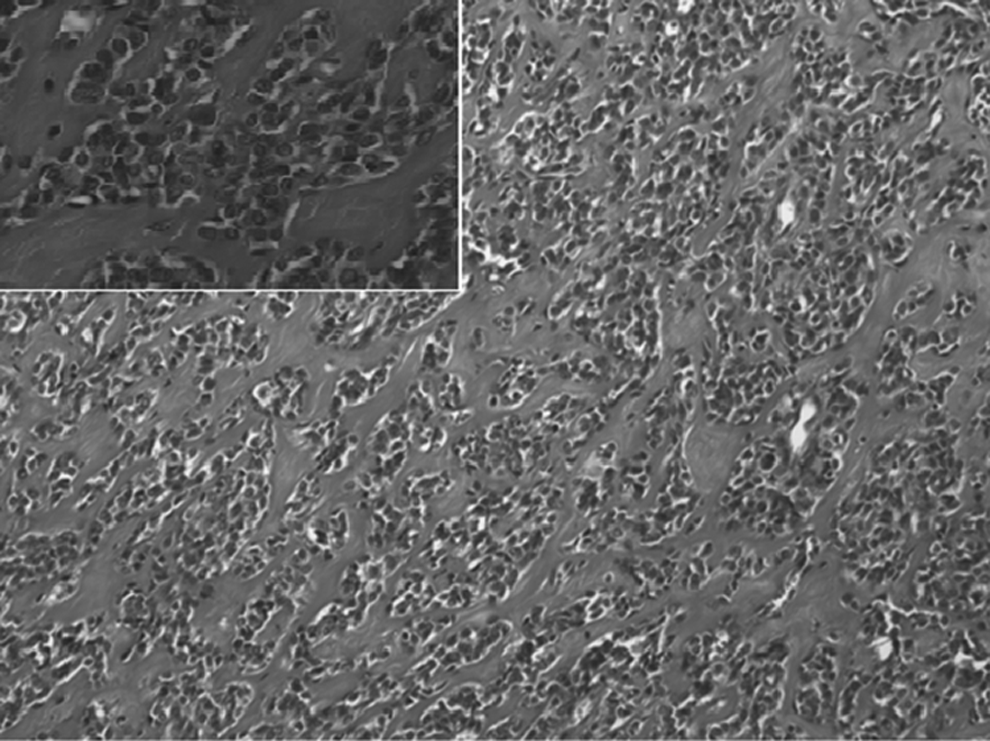
Cytologicallyepithelioid pattern described in case 3 (H&E,×20; inset: H&E ×40).
Immunohistochemical analysis performed in cases 3 and 4 showed smooth-muscle tumor cells with positive staining for desmin and caldesmon (Fig. 6). CD34 staining confirmed that there was no intravascular extension of the tumor in case 4. The glandular component of endosalpingiosis foci, noted in the fourth case, was positive for CK7 and negative for CK20.

Positive immunostaining of smooth-muscle tumor cells with desmin and caldesmon (inset).
There was no follow-up in cases 1 and 2. In case 3, the patient died during surgery. In case four, follow-up was for 10 months.
Discussion
Dissecting leiomyoma is an unusual variant of uterine leiomyoma defined by myometrial dissection. CDL is characterized by its macroscopic appearance resembling placental cotyledons. This tumor can extend to the extrauterine adnexal area with an exophytic pattern. However, recently, Roth et al. defined cotyledonoid leiomyoma as a new diagnostic term for benign smooth-muscle tumors with an exophytic growth pattern that did not demonstrate myometrial dissection. 2
CDL of the uterus, also called “grapelike leiomyoma,” is a very rare tumor among the wide variety of distinctive growth variants described in benign uterine leiomyoma. 3 It was first described in 1996 by Roth et al. in a series of four cases. 4 As they were collected by Dr. Sternberg who had originally studied the tumor as “a red seaweed lesion,” they were often termed “Sternberg tumors.” 3 Only 30 cases have been reported in the literature. 2 CDL of the uterus can present in a wide age spectrum ranging from 23 to 65 years with a mean age of 40 years. The most common clinical presentation consists of a pelvic mass and abnormal uterine bleeding. Large tumors are often observed, with an average size of 17.7 cm. 2
Several factors must be present to distinguish the gross appearance of a cotyledonoid leiomyoma. First of all, the leiomyoma must originate close to the serosal surface and extend into the free space of the pelvic cavity. Three of our four reported cases arose in the serosal side of the fundus. Second, the leiomyoma must exhibit a growth pattern in uterine leiomyoma characterized by dissection of the peripheral myometrium and presence of micronodules of swirled neoplastic smooth-muscle cells within the myometrium. 3 In the only example lacking an intramural dissecting component (case 3), the tumor was located at the interface between the myometrium and serosa, producing an exclusively exophytic growth pattern. Diagnosis in this case was based on the typical macroscopic appearance of numerous exophytic congested small nodules resembling placental cotyledons. Finally, the leiomyoma must show perinodular hydropic degeneration, which is a rare form of stromal change in leiomyoma characterized by the accumulation of edematous fluid in the connective tissue, subdividing the tumor into numerous, small, compact smooth-muscle nodules. The hydropic well-vascularized nodules can even resemble hemangioma. This particular appearance can cause diagnostic confusion with intravenous leiomyomatosis. 3 Hydropic degeneration was documented in cases 1, 2, and 3.
Malignancy-like appearance, which may lead to misdiagnosis, can be attributed to the alarming fungating features, the large size, and the appearing widespread infiltrative growth and frequent extension into the pelvic cavity and broad ligament. However, the histological features of this tumor show bland-looking leiomyoma with variable sized micronodules and disorganized and swirled neoplastic smooth-muscle fascicules. Fibrous or edematous markedly congested intervening stroma gives rise to the characteristic red-brown color of the nodules. 3 Marked atypia, mitotic activity, and coagulative necrosis are absent. 2 This type of tumor is often associated with perinodular hydropic changes, 5 endometriosis, or endosalpingiosis, and is usually discovered incidentally on macroscopic or microscopic examination.
Several histological variants of CDL are described in the literature, including cotyledonoid leiomyoma lacking the intramural component, intramural dissecting leiomyoma lacking the extrauterine component, cotyledonoid hydropic intravenous leiomyoma having the characteristics of CDL but associated with an additional intravenous component, and a variant displaying cytologically epithelioid pattern. 6 Some authors have suggested that frozen sections can be performed to avoid overtreatment and radical surgery during the reproductive age for such a potentially benign lesion. However, this is still controversial, since frozen-section diagnosis of smooth-muscle lesions is very difficult and can be disastrous. 5
Conclusion
In summary, CDL is a lesion that usually poses significant management and diagnostic challenges for gynecologists and pathologists with problematic differential diagnosis in microscopic evaluation. Meticulous histopathologic assessment should be performed in order to circumvent misdiagnosis and avoid overtreatment.
Although macroscopic findings of the tumors seem to indicate sarcoma, microscopic findings show them to be benign. Intraoperatively, the worrisome appearance of the gross specimen is often mistaken for malignant or nonuterine lesions, which may result in overtreatment.
Footnotes
Acknowledgments
We thank MSS Nazihaa Ben Ahmed for her technical help.
Disclosure Statement
No competing financial interests exist.