
Abstract
Abstract
Introduction
Case
This patient was a 45-year-old married woman with 7 children. She had had a late menarche at age 18 and an early menopause at age 35. She had no specific medical history, such as cancer or tuberculosis infection. She was complaining of metrorrhagia and dyspareunia for the last 5 years prior to presentation, with worsening of symptoms 4 months prior, along with vaginal discharge and pelvic pain. A clinical examination revealed a tumor and a circumferential ulcerative budding neck measuring 6 cm. The parametria and lymph nodes were not involved. A cervical biopsy revealed poorly differentiated squamous cell carcinoma. It proved to be invasive and was the cause of the surface ulcerations. Computed tomography (CT) revealed an abdominopelvic compressing tumor of the cervix without parametrium involvement (Fig. 1). The tumor was classified as IB2 (clinical lesions >4 cm in size), which was the indication for a radical hysterectomy and bilateral pelvic lymphadenectomy. The patient's preoperative assessment, including a chest radiograph, was normal. At the outset, it was surprising to note the presence of a low volume of liquid effusion containing fine granules that spread into the peritoneal space. At that moment, there was some hesitation regarding the surgical approach. However, the healthy appearance of the patient's uterus and its adjoining tissue, as well as the parametrium, and the absence of any noted surgical difficulty led to a decision to perform a radical hysterectomy, with removal of the ascitic fluid. A biopsy of the peritoneal granulations was also carried out. The pathology report revealed a huge anatomopathologic ulcerative neoplasm protruding 5 cm, filling the entire cervix and reaching the isthmus. The peritoneal samples revealed miliarylike granulations (Fig 2), with the largest measuring 0.5 cm.
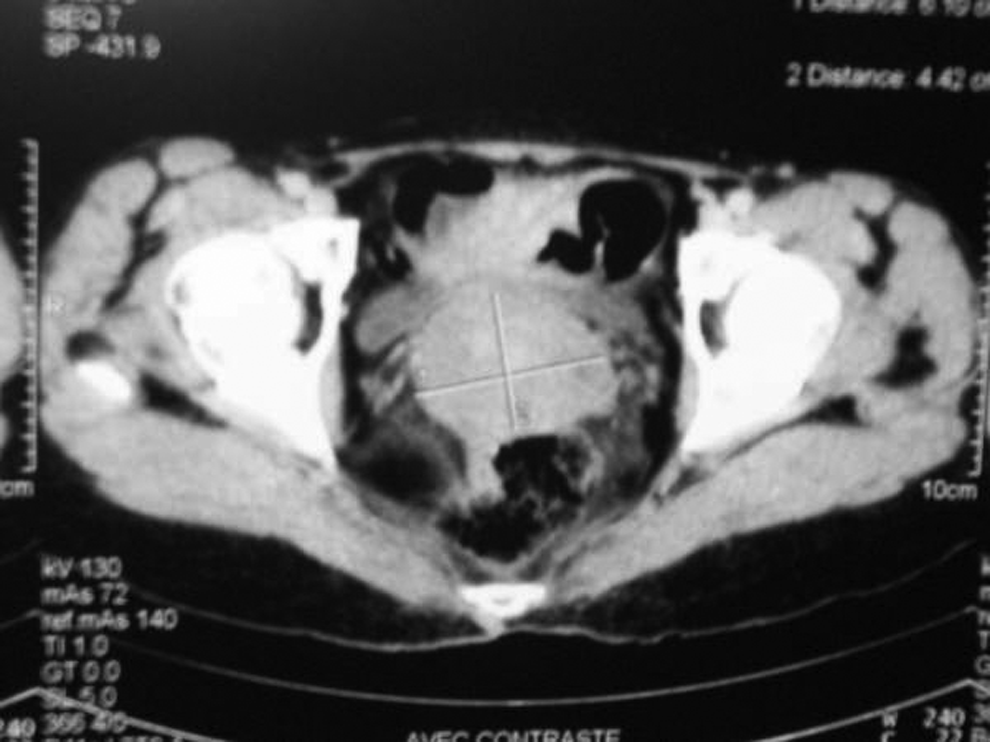
Computed tomography showing abdominopelvic compressing tumor of the cervix without parametrium involvement.
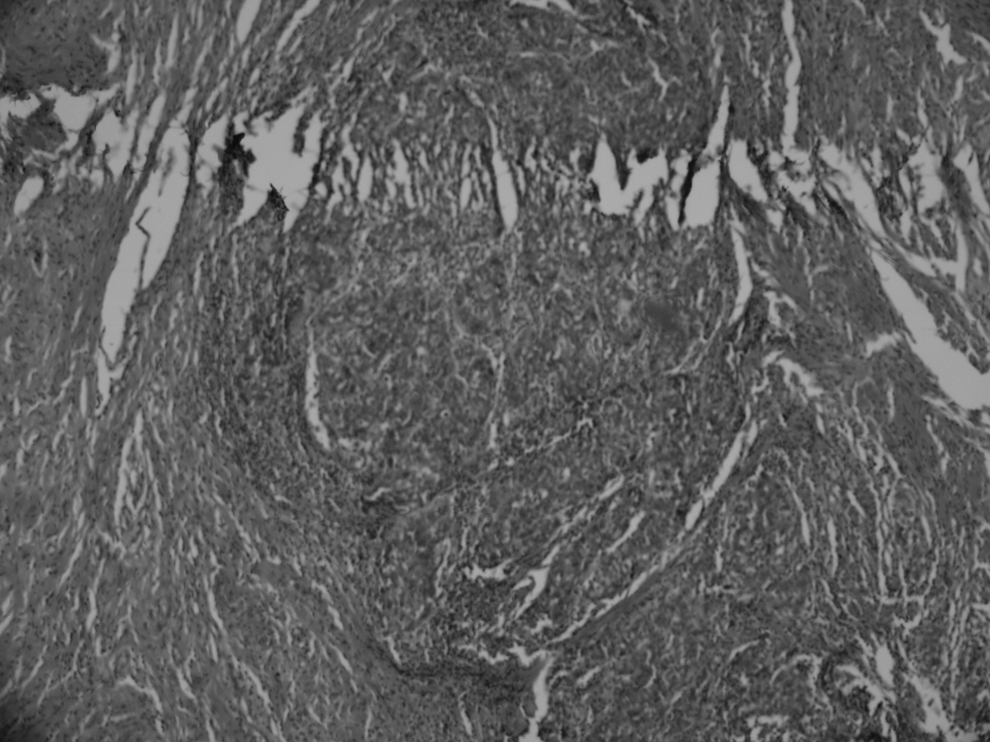
Miliarylikel granulations in biopsy sample.
Histological examination showed a syncytially structured carcinoma with squamous cells and mitotic figures. Picnotic cells were also noted. The stroma reaction was lymphocytic, with significant numbers of lymphocyte and plasmocyte elements that had areas of necrosis. The isthmus was also invaded. Vaginal margin samples taken on 2 cm of the anterior and 2.5 cm of the posterior, and the parametrium were not contaminated. The adnexa had a tuberculosis epithelial giant cell with caseous necrosis (Fig. 3). The peritoneum was the seat of the same necrotizing granulomatous inflammation. There was no lymph-node metastases in the ten nodes that were removed (the pelvic lymphadenectomy common and the external iliac nodes vein).
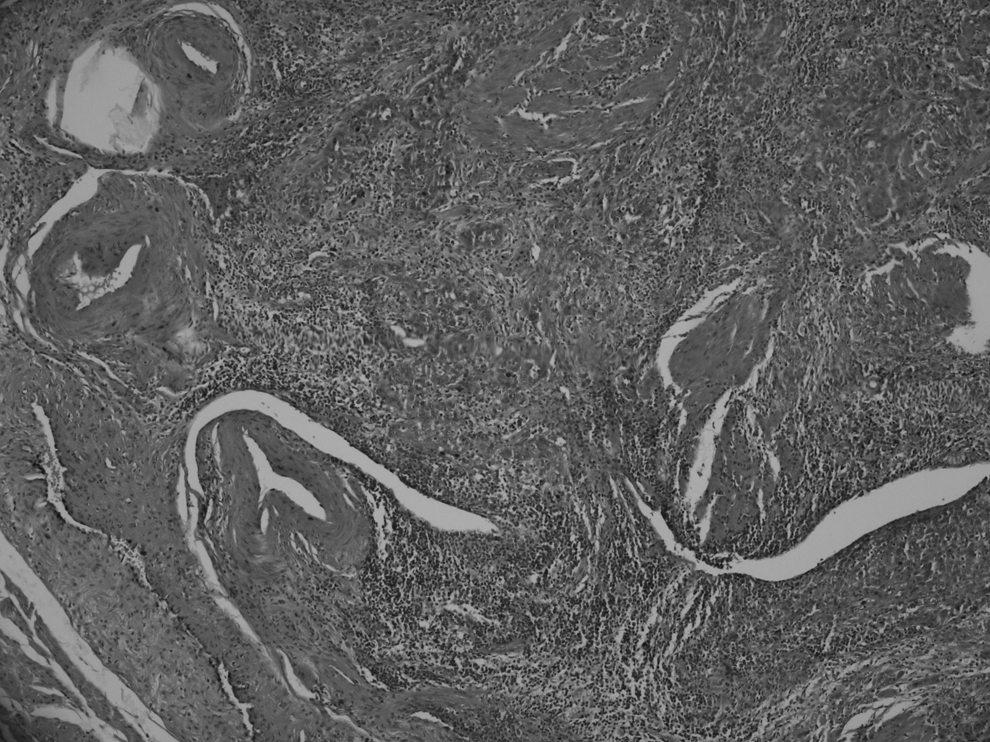
Adnexa has tuberculosis epithelial giant cell with caseous necrosis.
Finally, a diagnosis of squamous-cell type carcinoma of the cervix and genital and peritoneal tuberculosis was chosen. An immunohistochemical study showed a rise in CD4 and CD8 cells. As the immunolabeling for Epstein-Barr virus (EBV) was not conclusive, in situ hybridization was not done. A highly positive intradermal tuberculin reaction test was performed on the patient.
Results
The patient is currently receiving antituberculosis treatment.
Discussion
LEC of the cervix is a variant of squamous-cell carcinoma.3,4 It represents 0.7% of primary cancers of the cervix in women 3 and 5.5% of such cancers among Asian women. The pathogen is essentially EBV, 4 which is endemic in the people of Southeast Asia and in the Native Alaskan population. EBV's pathogenic role remains controversial. Human papilloma virus (HPV) is also a high-risk factor.5,6
This tumor is characterized by a proliferation in the endocervical canal, with an ulcerative burgeoning aspect, as occurred in the case of the current patient, in whom the tumor caused compression of the endocervix and its closing. The tumor is also characterized by a low tendency to metastasize. Indeed, in this patient, the tumor was classified IB2 and lymph-node dissection yielded negative results. Histologically, this cancer has a group of poorly differentiated tumor cells, with abundant cytoplasm surrounded by intense lymphocyte plasma-cell infiltration.3,4 Sometimes, this inflammation is so intense that it is necessary to use immunohistochemistry to confirm the presence of epithelial cells.
Because LEC has less tendency to metastasize, LEC is characterized by a better prognosis than squamous-cell carcinoma.
Abdominal tuberculosis represents 3%–10% of tuberculosis cases. Of the 596 cases of abdominal tuberculosis cited by Marshal, 7 peritoneal localization was found in 43%. This is an important cause of chronic pelvic inflammation and infertility in endemic areas. In addition, 11% of patients are asymptomatic. The diagnosis is mainly based on the culture of Mycobacterium tuberculosis (MTB). However, standard histopathologic criteria in tissue biopsies are now accepted.8,9 Two-thirds of tuberculosis cases are diagnosed based on the criteria of epithelioid granulomas and giant cells with caseous necrosis. The tuberculin test, positive in 55%–100% of cases, as well as the idea of tuberculosis contagion and hysterosalpingography can help determine the diagnosis. Ascites, when present, is exudative with a lymphocytic predominance, and the culture is positive in 20% of cases. Research using polymerase chain reaction (PCR) can isolate the MTB, but PCR's high cost and low sensitivity in 60%–80% 9 limits the spread of its use. This sensitivity becomes more effective if the culture is positive.
The prognosis is mainly based on the risk of irreversible infertility and chronic abdominal pain. The treatment is based on antituberculous agents.
The association between abdominal and genital tuberculosis and LEC is extremely rare. These two entities have in common lymphocyte proliferation and immunosuppression. This association creates diagnostic and therapeutic problems because ascites and peritoneal granulations encountered during peritoneal tuberculosis can be mistaken for peritoneal carcinomatosis associated with cancer. 10
This has delayed antituberculous treatment, as radiotherapy and chemotherapy were are prescribed first. Fortunately, in the current case, the CT scan did not reveal the existing peritoneal granulations. The same problem arises in cases of need for adjuvant radiotherapy. The latter must be delayed, because concomitant use of antibacterial treatment is contraindicated.1,11 The third worry concerns the prognosis. Even LEC has a good prognosis, but its occurrence, as seen on pathology (such as tuberculosis), decreases body immunity.
Conclusions
In an country such as Morocco, tuberculosis is endemic and is still mentioned as a differential diagnosis of cancers especially gastrointestinal and ovarian cancers, when surgical exploration is necessary for histologic diagnosis. LEC of the cervix is a rare entity, and its association with genital and peritoneal tuberculosis is even rarer. The treatment must be oncologic as well as antibacterial, which is a challenge especially in advanced stages.
Footnotes
Disclosure Statement
No financial conflicts exist.