
Abstract
Abstract
Introduction
Materials and Methods
Seventy-nine patient charts from January 2010 to June 2011 were reviewed retrospectively from one surgeon who practiced for 28 years in a private practice. No residents were involved in these cases. No patients were excluded from the study except those requiring ancillary procedures such as vaginal vault or rectocele repair at the same time of the laparoscopic-assisted vaginal hysterectomy (LAVH) procedure.
Group A involved cases in which the Enseal Trio Device bipolar tissue and coagulation cutting forceps with 3-mm tip was used for the laparoscopic portion. A 5-mm umbilical port was inserted for the camera, and two lateral 5-mm ports for a grasper and the Enseal Trio Device. Ovarian pedicles or utero-ovarian pedicles were grasped, cauterized, and cut with the Enseal Trio Device, depending whether ovaries were being removed or left in situ. Then, vaginally, a posterior colpotomy was performed. After injection with 1% lidocaine with epinephrine, the cervix was circumscribed and advanced using sharp dissection. The uterosacral ligaments were clamped, cut, and tied with 0-Vicryl. Using the 14-cm Enseal Trio Device 3-mm cutting cautery device, the cardinal ligaments and uterine vessels were sealed and transected. Anterior colpotomy was made using Metzenbaum scissors and the specimen was then removed through the vagina. The posterior cuff was then baseball stitched with 0-Vicryl. A McCall stitch incorporating the uterosacral ligaments and the posterior cuff was done using 0-Vicryl to help prevent future enterocele. A purse-string suture of 0-Vicryl was used to close the peritoneum, followed by a 0-Vicryl interlocking baseball stitch to close the vaginal mucosa. All patients received prophylactic antibiotics 1 hour prior to surgery.
In Group B, the abdominal portion of the procedure was done following the same steps, using a 3-mm, 35-cm Enseal Trio Device through two lateral 5-mm ports. Then vaginally, the cervix was injected with 1% lidocaine with epinephrine. The cervix was circumscribed and advanced using sharp dissection. A posterior colpotomy was made with scissors. The uterosacral ligaments were clamped, cut, and tied with 0-Vicryl. The cervix was circumscribed and advanced with sharp dissection. Then the cardinal and uterine vessels were clamped, cut, and tied with 0-Vicryl bilaterally. An anterior colpotomy was made, and uterine specimen was removed. The posterior cuff was baseball stitched with 0-Vicryl. Then a McCall stitch of 0-Vicryl was used incorporating the uterosacral ligaments and posterior cuff to help prevent any future enterocele. The perineum was then closed with 0-Vicryl continuous purse-string suture, and the vaginal mucosa was closed with a 0-Vicryl baseball stitch. Postoperatively, the patients in both groups received hydromorphone HCl (dilaudid intravenously), followed by oxycodone HCl (percocet), unless allergies were present. Patients were discharged home the following morning with instructions for follow-up in the office in 3 weeks.
Once Group A and B were established, chart review was completed for data collection of the following:
(1) Estimated blood loss, determined on the basis of the anesthesia record; if anesthesia record was not marked, then surgeons' estimated blood loss used (2) Operating time, defined as period from beginning of incision in the umbilicus abdominally to conclusion of the vaginal portion of the procedure, using the vaginal mucosa stitch (3) Hospital stay, defined from day of surgery to, and including, day of discharge (4) Postoperative fever >38°C (5) Postoperative bleeding (6) Return to the operating room (7) Readmission to the hospital within 1 week (8) Uterine weight obtained from a pathology report (9) Patient weight in kg.
Statistical analysis of all parameters was performed using unpaired two-sample t-tests. IRB approval was obtained through the Medical Affairs Department of Glens Falls Hospital.
Results
A total of 79 patient's charts were reviewed. Each patient was placed into either group A or group B. Group A consisted of 44 patients who underwent an LAVH±bilateral salpingo-oophorectomy (BSO) with the Enseal Trio Device used both laparoscopically and vaginally. Group B consisted of 35 patients who underwent LAVH±BSO with the Enseal Device Trio laparoscopically and suture ligation vaginally.
The surgical time for patients who received a LAVH±BSO with Enseal laparoscopically and vaginally was significantly lower than that of patients who received identical procedures with conventional vaginal suturing (Fig. 1). The mean surgical time for LAVH±BSO in Group A (Enseal Trio Device) was 52.4±14.4 minutes, while it was 63.7±14.9 minutes for conventional vaginal suturing (Group B). The difference of 11.2 minutes in mean surgical time was highly significant (P=0.001). This translates into a 19% savings in surgical time.
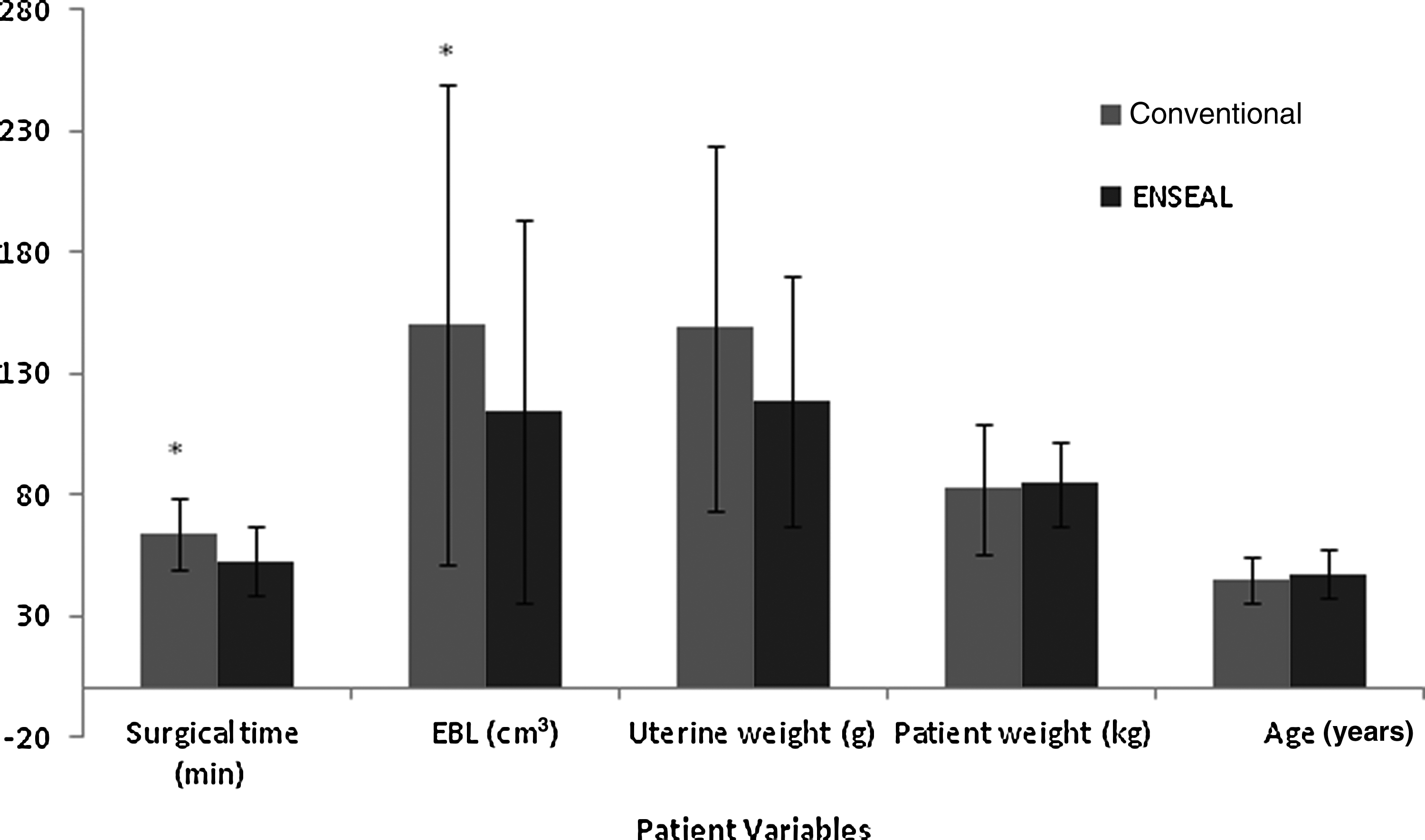
The average surgical time, estimated blood loss (EBL), uterine weight, patient weight, and age of patients (±standard deviation) who received a laparoscopic-assisted vaginal hysterectomy with or without bilateral salpingo-oophorectomy (LAVH±BSO). The conventional treatment included patients who received a LAVH with suturing (n=35), whereas treatment with the Enseal® Trio Device (Ethicon Endo-Surgery, Inc., Cincinnati, OH) included patients who received a LAVH with the cauterizing instrument (n=44). An asterisk (*) denotes significant difference between conventional and Enseal treatments as measured by unpaired two-sample t-tests (p<0.05). min, minutes.
Intraoperative blood loss as assessed by the anesthesia records was lower in the Enseal Trio device group than in the control group, as shown in Figure 1. The Enseal Trio Device group blood loss (114±79.1 cm3) was significantly lower than that of the patients who received their surgeries with conventional suturing techniques (150.00±99.2 cm3; p=0.049). No patient required a blood transfusion. Uterine weight (in g), patient's weight (in kg) and age (in years) all showed no significant difference between the conventional suturing technique and the Enseal Trio Device group (Fig. 1). Hospital stay was identical for both the Enseal Trio Device group (24 hours) and the control group (24 hours). There were no postoperative complications in either the Enseal Trio Device or the conventional suturing group. Parameters evaluated included postoperative fever >37°C, postoperative bleeding, return to operating room, and readmission to the hospital within 1 week.
Discussion
Hysterectomies are one of the most common gynecologic surgeries, with approximately 600,000 performed a year in the United States. 9 Surgeons are always seeking improvements in techniques that improve the patient's surgical experience.
Surgical time for the Enseal Trio Device was 19% lower than for the suturing technique. Other research has reported similar results.2–6 There are five randomized control trials comparing bipolar vessel sealing with conventional suture ligature in vaginal hysterectomy. Levy and Emery compared LigaSure device to sutures with statistical significance shown with respect to a decrease in operating room (OR) time and a decrease in intraoperative blood loss. 6 Zubke et al. evaluated the BiClamp Device and showed a 21% decrease in OR time and decreased blood loss. 9 Hefni et al. 4 and Cronze and Coning 1 showed similar results. A labial burn was the only complication noted in two studies. Of note, the devices used in all of these studies are larger than the Enseal Trio Device, with a tip of 5 mm and a larger lateral thermal spread than 1 mm.
Because of the unique properties of the Enseal Trio Device and the corresponding radiofrequency generator, lateral heat spread is only 1 millimeter. Only the Harmonic scalpel has such minimal lateral spread, but it does not seal vessels up to 7 mm.
The narrow 3-mm curve tip of the device can be easily placed in an anatomically narrow pelvis where placing suture needles could be troublesome. Of note, no skin burns occurred in the series.
Other parameters evaluated did not show statistical significance (patient's weight, uterine weight, age). Complication rates were the same for both techniques. Cost analysis at this hospital showed anesthesia time to be $300 per hour, and operating room time at $2,000 per hour, and 0-Vicryl sutures to be $1.62 per suture. One can use the 35-cm laparoscopic Enseal Trio Device vaginally for no added cost; however, the 14-cm device is easier to use vaginally. This would add $397 to the case. With a 19% reduction in OR time, anesthesia time, and eight less 0-Vicryl sutures for a cost reduction of $449.96, there is still a $52.96 financial benefit for the complete Enseal Trio Device technique.
Further research in engineering of the Enseal Trio Device evaluating the use of one handle with two interchangeable shafts may further decrease equipment costs.
Conclusions
The Enseal Trio Device (a bipolar tissue, sealing, and cutting device) reduces procedure times and blood loss. It has a narrow, curved, 3-mm tip with 1-mm lateral thermal spread that seals vessels up to 7 mm. By sealing both sides of the vessels, blood loss is less than in conventional suturing techniques. OR surgical times were decreased by 19%, using Enseal Trio Device vaginally when compared to conventional suture techniques. Decreased OR time increases physician and staff efficiency and exposes the patient to less anesthesia and potential complications. Cost analysis shows savings using the Enseal Trio Device technique. Using Enseal Trio Device laparoscopically and vaginally is a user-friendly technique with positive benefits for patients with respect to blood loss and OR surgical time.
While other studies compare the use of bipolar devices in vaginal hysterectomies, the authors believe this study proves the efficacy of these devices in the vaginal portion of LAVH procedures. These results show that bipolar devices, especially the small tip design of the Enseal Trio, can provide improved access to the cardinal ligaments and uterine vessels in these cases where a large or fibrotic uterus may prove more difficult with the standard suturing technique. The added cost of an additional device is a common objection. The reduced OR time and elimination of sutures actually reveals a cost savings for the hospital even with the use of two separate devices for the abdominal and vaginal portions of the procedure. Overall, the study proves that the use of a second advanced bipolar device during the vaginal portion of an LAVH is effective at reducing OR time and blood loss without added cost.
Footnotes
Acknowledgments
This study was supported by an educational grant from Johnson and Johnson.
Disclosure Statement
The authors have no commercial, proprietary, or financial interest in the products or companies described in this article.