
Abstract
Abstract
Introduction
What makes the current case unusual is the surgical approach. The tumor was completely resected via laparoscopy. To the current authors' knowledge, this is the first case of a laparoscopic resection of a lipoleiomyoma.
Case
This article reports a case of a 41-year-old woman, gravida 3, para 1, who presented with abdominal discomfort, dysmenorrhea, and menorrhagia. The patient reported these complaints for 1 year, and the symptoms had gotten worse in the previous 4 months before being referred to the hospital for further management. Her past surgical, gynecologic, and medical histories were unremarkable. In the outpatient department, a pelvic examination revealed a normal cervix and an abnormal mass occupying the cul-de-sac. No adnexal masses were palpated. The transvaginal sonography (TVS) revealed a posterior uterine wall or cul-de-sac mass with a markedly hyperechoic appearance, measuring 7 cm (Fig. 1). The endometrial stripe was normal and no uterine biopsy was performed. The diagnostic impression was extrauterine leiomyoma, lipoleiomyoma, or rectum tumor. Because of the possibility of rectum involvement—but also because of the ultrasound features of the mass—an abdominal and pelvic computed tomography (CT) scan was done. It showed a subserosal uterine myoma from the cervical region, chiefly composed of fat-density tissue, with adjacent rectum compression (Fig. 2). Laboratory data revealed only microcytic anemia (hemoglobin level of 10.1 g/dL and a mean corpuscular volume of 76.4 fL). Because of this patient's persistent abnormal uterine bleeding and her radiographic findings (an abnormal mass over the uterine lower corpus), laparoscopic myomectomy was carried out after discussion with the patient. A 10-mm laparoscope was inserted through her umbilicus. Three 5-mm accessory trocars were inserted for ipsilateral two-handed surgery and for the assistant. A subserous myoma with intramural component measuring 6×4 cm was found on the lower uterine segment (Fig. 3). The myoma was enucleated by traction (on the myoma) and with coagulation of the feeding vessels. The uterine incision was then repaired: the first layer with two extracorporeal “fisherman's” knots and the second layer with intracorporeal reverse interlocking suture, using 1-0 Monocryl. Posterior culdotomy was performed followed by myoma delivery. The vaginal incision was repaired with a continuous 1-0 Vicryl suture.

Transvaginal ultrasound revealing a well-limited hyperechoic mass in the posterior wall of the uterus.

Computed tomography showing a mass with fatlike density.

Protruding mass over the lower uterine segment (black arrow).
Results
Microscopically, the tumor proved to be a lipoleiomyoma, and the histologic examination showed sections of fascicles of smooth-muscle cells with lobules of mature adipose cells and focal myxoid degeneration (Fig. 4).
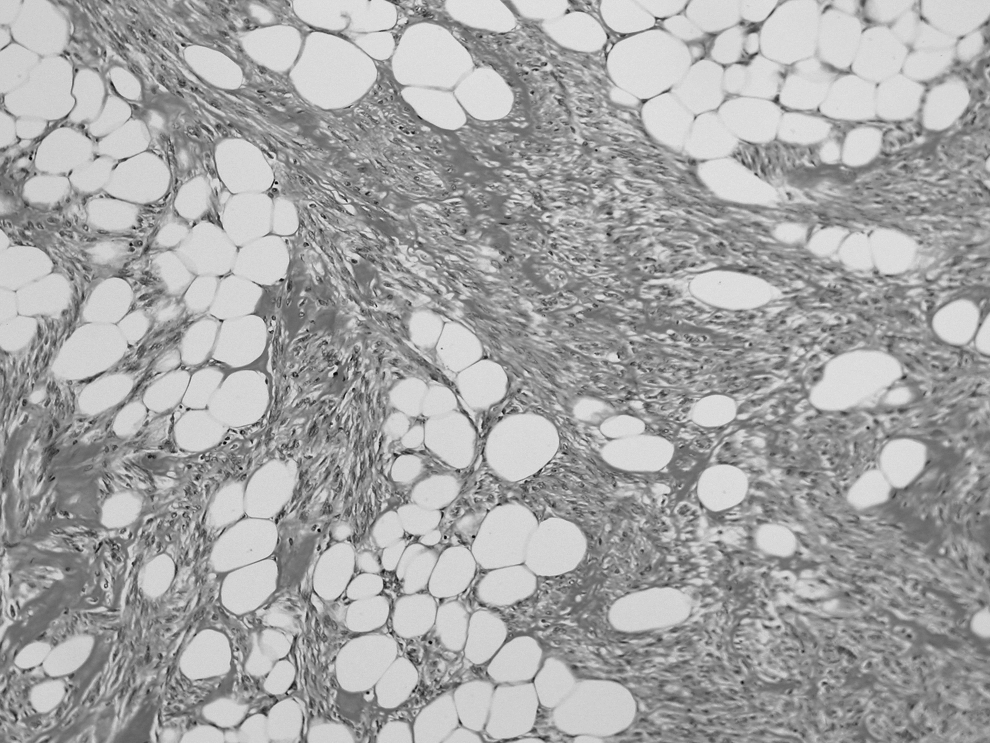
Histologically, the tumor consisted of smooth-muscle cells and mature adipocytes (H&E 100×).
During follow-up, 3 months after the surgery, the patient recovered well and the abnormal uterine bleeding resolved.
Discussion
Uterine lipoleiomyoma is an unusual entity. In the literature, the incidence ranges from 0.03% to 2.1% of all patients undergoing hysterectomy for leiomyomas; however, they can be more prevalent than previously supposed.1–4 There are several reasons for this fact: lipomatous tumors are easily neglected in some incidentally discovered cases because of their benign nature; asymptomatic lipoleiomyomas are likely to remain undetected; and the lipomatous component is often misinterpreted as artifact or as vessel space.
Most lipoleiomyomas have an intramural location, and they are often identified in the uterine corpus, but they may also arise in the cervix, broad ligament, round ligament, omentum, and even in the retroperitoneum. 1
When they are symptomatic, lipoleiomyomas mimic the symptoms of leiomyomas. Thus, pelvic pain, abdominal fullness, dysmenorrhea, and menorrhagia are the main complaints.
The pathogenesis remains unclear, and many hypotheses have been proposed, ranging from changes in lipid metabolism to fatty infiltration of connective tissue. However, fatty metamorphosis of the smooth-muscle cells of a leiomyoma seems a more likely origin of lipoleiomyoma rather than fatty degeneration.1,2 In one study of 50 cases published by Wang et al., the benign nature of lipoleiomyomas was confirmed after 5 years of follow-up. 1 The researchers also reported that all lipoleiomyomas in their series were composed of mature adipocytes. Histology revealed no mitotic activity, no lipoblasts, no atypia in either adipocytes or smooth muscle cells, and no presence of necrosis in any case. These findings are also supported by another study published in 2004. 5
Conclusions
Different imaging modalities may play an important role in determining the fatty nature of the mass. In the current case, the TVS findings were unusual, mainly because of the hyperechoic appearance of the suspected leiomyoma; however, the CT scan showed a well-circumscribed, predominantly fatty mass with some areas of nonfat soft tissue. MRI findings can also be important for defining the fatty nature of lipoleiomyomas. 2 High signal intensity on T1- and T2-weighted images and chemical shift artifacts within the lesion are all characteristic features of masses that have a lipomatous nature.
Differential diagnosis may include ovarian teratomas, spindle cell lipoma, angiolipoma, and leiomyoma with fatty degeneration, atypical lipoma, and well-differentiated liposarcoma.
According to the literature, the current case is infrequent because of the surgical approach (laparoscopic myomectomy).
Footnotes
Disclosure Statement
No competing financial conflicts exist.