
Abstract
Abstract
Introduction
In this report, the case of a uterine myoma is described in a 14-year-old girl who presented with lower abdominal and back pain and irregular menses.
Case
A 14-year-old white female patient was referred to our Department because of menstrual disorders (menorrhagia), and abdominal and back pain. Her family, past medical and surgical history was unremarkable. Menarche occurred at 11 years of age; she had irregular and heavy menstrual periods, lasting up to 6 days; the patient had no dysmenorrhea. The patient had never used the oral contraceptive pill or other hormonal therapies. Abdominal examination revealed a large mass extending 3 cm above the umbilical transverse line. A vaginal examination was not performed because the patient was a virgin. Rectal examination confirmed the presence of a large, round mass with a tense-elastic consistency, which seemed to originate from the posterior uterine wall.
Hematological and biochemical parameters were normal. There was no sign of systemic infection (temperature 36.6°C; white blood cells [WBC] 6.90×10,000/mm3; polymerase chain reaction [PCR] and erithrocyte sedimentation rate: negative). Tumor markers (including inhibin, Ca 19.9, Ca 125, α-fetoprotein, lactate dehydrogenase LDH, and β-human chorionic gonadotropin) were normal.
Abdominal ultrasound revealed a large mass (15×13×10 cm) that was quite homogeneous and isoechogenic to the myometrium; there was a small amount of free fluid in the pouch of Douglas. At Doppler images, the vascularization was mainly peripheral. Magnetic resonance imaging (MRI) showed an anteverted uterus with a large solid mass, relatively homogeneous in T1-weighted and T2-weighted images, which originated from the myometrium of the posterior uterine wall (Fig. 1). This mass displaced the uterine cavity; there was no evidence of rectal compression. On the basis of the imaging findings, surgery was judged to be required.

Magnetic resonance T2-weighted image showing the uterine myoma.
An intramuscular injection of leuprolide acetate (3.75 mg, Decapeptyl, Ipsen, Rome, Italy) was administered about 3 months before surgery in order to reduce the volume of the mass and decrease the intraoperative blood loss. Twenty-two (22) days after the first injection of leuprolide, the patient was admitted again to our department because of high temperature (39.6°C), leukocytosis (WBC 15.90×10,000/mm3), high PCR (125 mg/L), and intense abdominal pain of increasing severity. Surgery was performed on the day after the admission to the hospital. A Pfannenstiel transverse laparotomy was performed. The uterus had increased volume because of the presence of a large intramural mass in its posterior wall (Fig. 2). Postphlogistic adhesions were present between the posterior uterine wall and the small bowel. Hematic free fluid was collected in the pouch of Douglas and sent for cytological examination. Myomectomy was performed by a vertical incision in the posterior uterine wall; the endometrial layer was not opened. The uterine wall defect was sutured in four layers. The postoperative course was uneventful.

Enucleation of the uterine myoma by Pfannenstiel transverse laparotomy.
At pathologic examination, the mass appeared as a typical myoma (spherical, red–tan, soft tissue). It weighted 480 g, measured 13×10×10 cm, and was covered by a fibrous pseudocapsule beneath which a thin venous net was present. On cut section, the mass had a fasciculated appearance with a red wine color and soft consistency. There were hemorrhagic and necrotic areas. Microscopic examination revealed a leiomyoma with bundles of fusiform cells and focal areas of myxoid degeneration and sclerohyalinosis; there was no sign of malignancy (mitotic count <5/10 high-power field [HPF]). Immunohistochemical staining showed strong and diffuse positive staining for desmin, medium and diffuse staining for smooth-muscle actin, and low-medium and focal staining for S-100. Ki67 was positive in the 1%–2% of neoplastic cells and the Ki67 mitotic index was 1/10HPF (Fig. 3). The cytological examination of the fluid found in the pouch of Douglas revealed no malign tumor cells. Therefore, all the examinations confirmed the benign nature of the uterine mass.
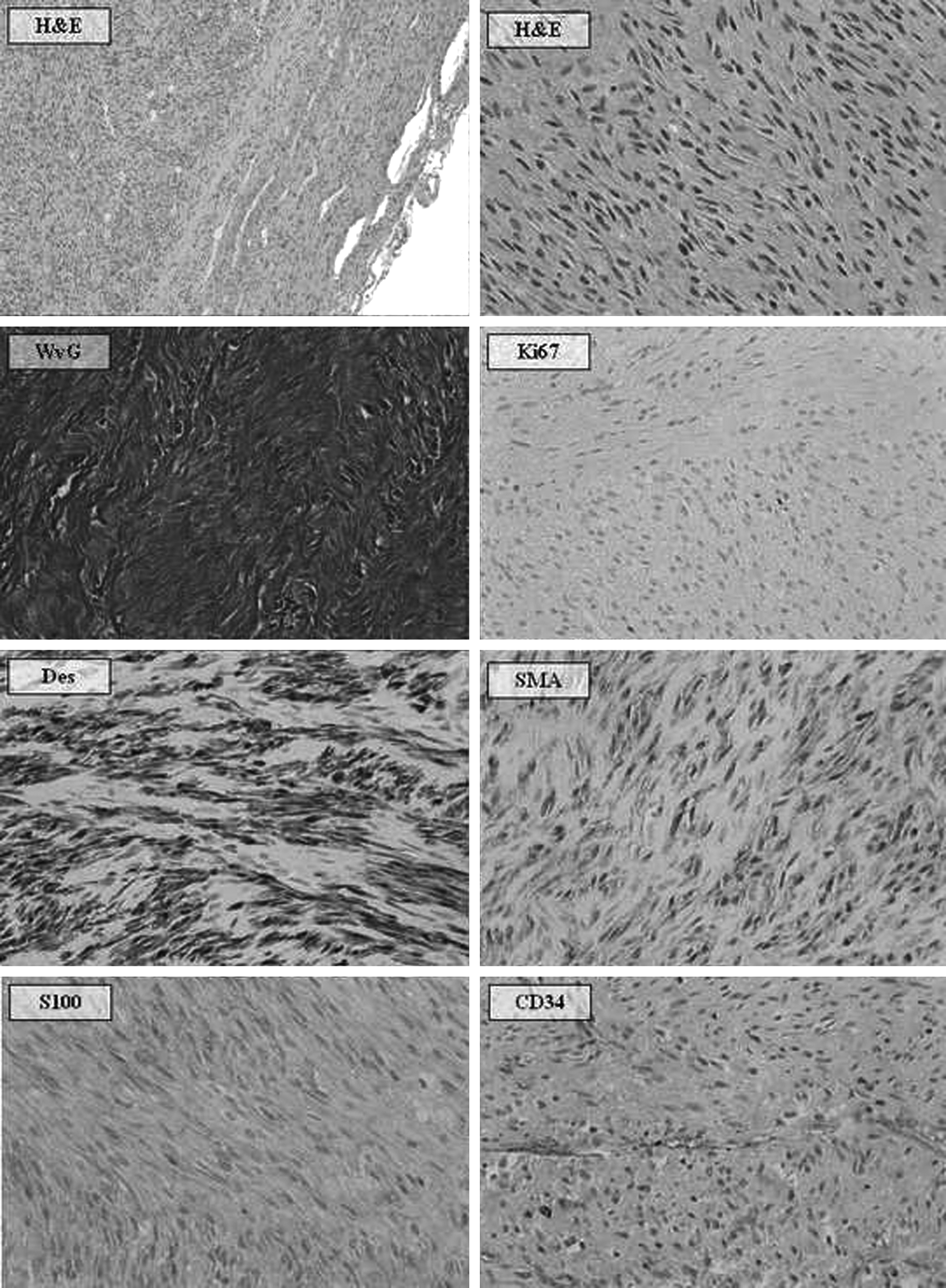
Microscopic and immunohistochemical examination.
Results
At follow-up, the patient reported heavy vaginal bleeding at the first menstrual period after surgery followed by regular and painless menses. Ultrasonography performed at 6 weeks, 3 months, 6 months, 1 year, and 2 years from surgery demonstrated an average-sized uterus and no recurrence of myoma.
Discussion
At presentation, uterine myomas may be asymptomatic (30%–80% of cases), but abdominal and back pain, compression symptoms, and vaginal bleeding with anemia are frequently present at diagnosis. Fields and Neinstein 6 compared the first clinical presentation of uterine myomas in adolescents with the presenting symptoms in the adults. 16 They observed that, in adolescents, 30% of myomas are asymptomatic (50%–80% in the adults), 50% cause menstrual abnormalities (30% in adults), and urinary abnormality is less frequent than in adults (5% in adolescents versus 20% in adults). In their series of 10 patients younger than 21 years of age, 40% of the patients also had symptom of compression and 20% had back pain.
The patient in the current report required surgery because of fever and increasing abdominal pain. Obviously other conditions may cause these symptoms such as appendicitis, hemorrhagic corpus luteum, adnexal torsion, and ectopic pregnancy. However, our patient was a virgin and previous radiological imaging suggested the diagnosis of uterine myoma.
The preoperative workup is particularly relevant in adolescents because fertility sparing and low surgical injury are mandatory in this population. Clinical examination, abdomino-pelvic ultrasound, computed tomography (CT), and MRI are commonly used in the differential diagnosis of pelvic masses and uterine myomas. Obviously, ultrasound is the first-line imaging technique used to evaluate a pelvic mass because of its availability and safeness. The second-line imaging techniques are CT and MRI, the latter being the most effective technique to evaluate uterine myomas.17–23 When myomas are typical with no sign of degeneration, they appear at MRI as homogeneous and they have hypointense signal. However, myomas may have a variety of degenerations (myxoid, hyaline, hemorrhagic, cystic, fatty, calcified) and degenerated myomas have heterogeneous signal intensity on MRI. In the presence of rapid growth of the mass, signs of degeneration on MRI, free fluid in the pouch of Douglas or ascites, a differential diagnosis with malignancies (such as leiomyosarcoma) should not be neglected. MRI has a specificity, sensitivity, positive predictive value, negative predictive value, and diagnostic accuracy of 93.1%, 100%, 52.6%, 100%, and 93.1%, respectively, in differentiating benign myomas from uterine sarcomas; these values increase to 93.8%, 100%, 83.3%, 100%, and 95.2% with dynamic MRI alone, and 100%, 100%, 100%, 100% and 100% with combined use of LDH and MRI. 24 Another study suggested that the combined use of T2-weighted and diffusion-weighted MRI for the differentiation of uterine sarcomas and benign myomas allows a specificity and sensitivity of 100% to be obtained. 25 In the current patient, MRI demonstrated a homogeneous mass without signs of degeneration, confirming the suspicion of benign uterine myoma, and it was decided that more advanced imaging techniques were not required. The myomectomy was performed by laparotomy because of the mass size; in addition, our patient was a virgin, thus preventing the use of a uterine manipulator during laparoscopic myomectomy.
Only an accurate pathological examination of the mass, including immunohistochemistry, allows a differential diagnosis between benign myomas and low-grade sarcomas. Increased cellularity, nuclear atypia, and increased mitotic activity are features that can be found in an adolescent population and suggest the need to carefully evaluate the tumor to exclude malignancy or malignant transformation. Other common features that should be carefully examined are tumor cell necrosis, atypical mitotic figures, infiltrative borders and, in a minority of cases, vascular invasion. Immunohistochemistry (positivity for smooth-muscle markers such as desmin and h-caldesmon) may facilitate the diagnosis of poorly differentiated tumors. 26 The rapid growth and uncommon large size of uterine myomas, as in this report, may also be associated with malignant transformation. 11 However, up to now, no case of uterine leiomyosarcoma has been reported in adolescents and they are very rare under the age of 30 years. 27
The management of myomas can be conservative, medical or surgical. If myomas are small and asymptomatic or well controlled with hormone therapy, observation can be enough. Surgical treatment is necessary if symptoms are present and evolve or if the mass has a rapid growth. Myomectomy must be the first choice because preservation of fertility is the main factor for the adolescent population.
The administration of gonadotropin-releasing hormone agonist (i.e., leuprolide) may be useful to temporarily control the menstrual disorders; in addition, it may decrease the size of the myoma, minimizing intraoperative blood losses and facilitating fertility-sparing surgery. 28 In the present patient, the administration of leuprolide acetate was followed by an increased severity of abdominal pain associated with biochemical evidence of inflammatory reaction, which required anticipating surgery. It can be hypothesized that the administration of leuprolide acetate caused acute ischemia of the large uterine myoma.
The follow-up of these young patients is another important element that should be carefully considered. In our case, at 2-year follow-up no recurrence was diagnosed. A recent report demonstrates that, even if it is extremely rare, recurrence after surgery is possible and should not be ignored. In that case, a 14-year-old patient underwent an abdominal myomectomy for a 16-cm myoma, but after 1 year the mass recurred and the patient was operated on again through a robotic myomectomy for an 11-cm myoma; after another year, the mass had recurred again and been stable at 3 cm in size and the patient felt no symptom. 15
Conclusions
Myomas are rare in those in the pediatric and adolescent age groups; they should be considered in girls with abdominal/back pain, menstrual disorders, and vaginal bleeding.
This report confirms that large uterine myomas may be diagnosed in adolescents. Before surgery, combining ultrasonography with MRI permits precise information to be obtained on the nature of the mass. Fertility sparing and low surgical injury are mandatory in this population.
An accurate pathological examination, including immunohistochemistry, of the mass is fundamental to exclude malignancies even if, up to now, no case of uterine leiomyosarcoma has been reported in adolescents, and they are very rare under the age of 30 years. 27
Footnotes
Disclosure Statement
The authors have no potential conflict of interest to disclose.