
Abstract
Abstract
Introduction
Case
The patient, a 30-year-old black African woman, primigravida and nulliparous, had a history of abortion at 3 months of pregnancy, regular menstrual cycles since menarche at age 13 years, and 5 days' duration of menstruation. It is also noted that she had underwent a difficult myomectomy with opening uterine cavity in a private medical center on June 9, 2011 by a general surgeon. Several incisions were made on the uterus with removal of several myomas. The postmyomectomy period was complicated with severe wound sepsis that resumed a month later. She consulted the authors' department on November 4, 2011, 5 months after myomectomy because of the appearance of cyclical monthly bleeding through the myomectomy abdominal scar. She also had bleeding vaginally for the same duration (5 months) and at the same time as abdominal bleeding.
The patient's general physical examination was unremarkable. Her pelvis was soft, without pain or mass. At the Pfannenstiel scar near the midline, there was a sinus opening of about 4 mm through which blood flows monthly (Fig. 1). On speculum examination, her cervix and vagina were healthy looking. On vaginal examination combined with abdominal palpation, the uterus was subnormal in size and mobile. Given these signs, uterocutaneous fistula was suspected.

The arrow indicates the 4-mm cutaneous sinus openings on the Pfannenstiel scar through which the menses flowed.
When methylene blue was injected into the cervix, it was seen flowing from the cervix to the abdominal wall sinus. At hysterosalpingography (HSG), there was bilateral tubal patency; a fistulous tract was characterized by an additional image extending from the uterine fundus out to the skin (connecting the endometrial cavity with the skin; Fig. 2). An exploratory laparotomy performed on February 21, 2012 showed that the uterus was densely adherent to the rectus muscle and to the anterior abdominal wall. Preoperatively, the abdominal cavity was intact. A uterine fistula of approximately 4 mm with granular edges was demonstrated and was at the front of the uterus (Fig. 3).
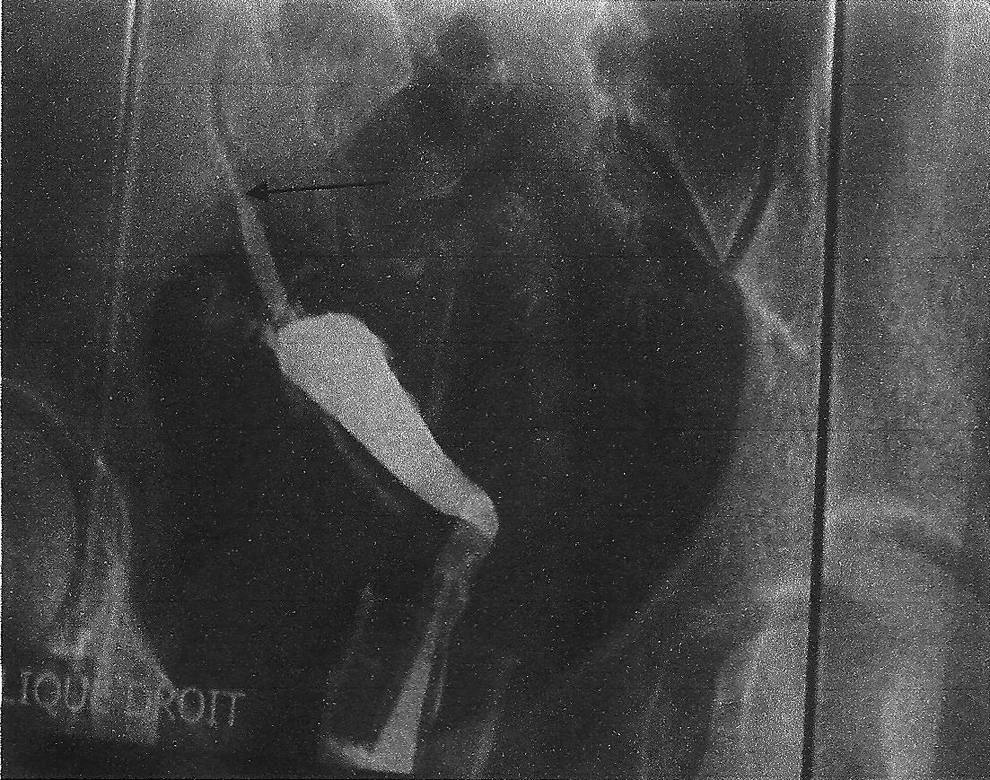
Hysterosalpingography. The arrow indicates the fistulous tract extending from the uterus fundus to the abdominal anterior wall. There is bilateral tubal patency.
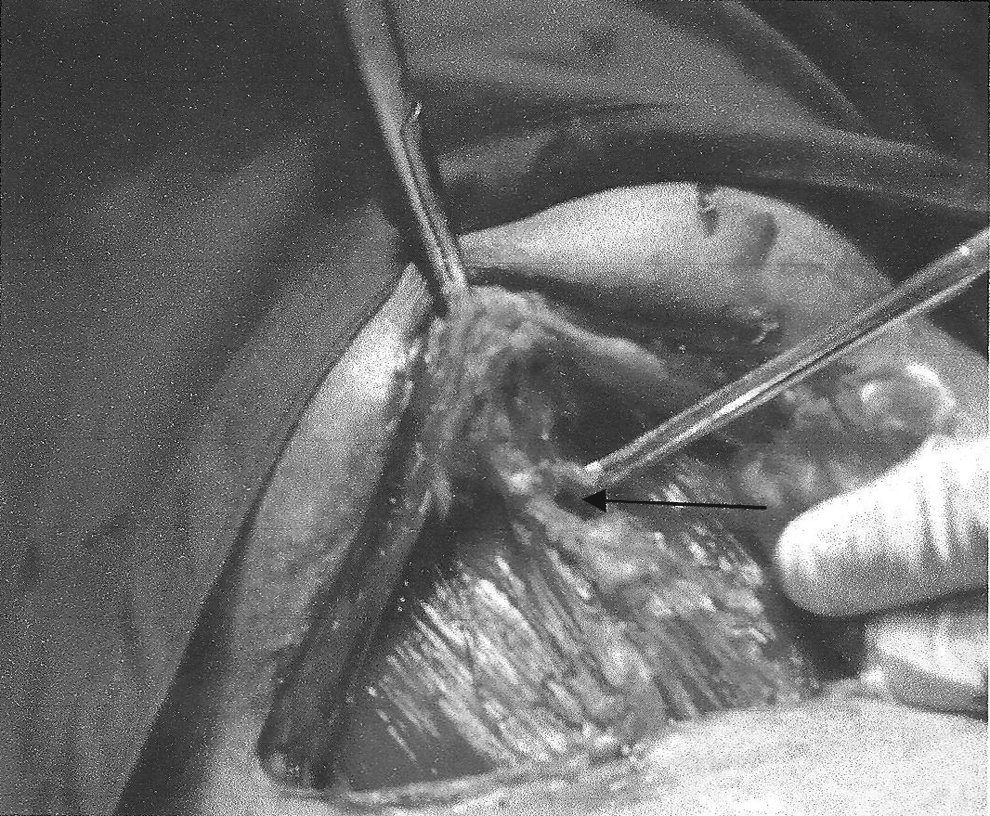
The arrow indicates the orifice of the fistula intraoperatively, which was at the front of the uterus. Note the granular edges.
The fistulous tract was excised completely followed by a uterine suture with 1–0 Vicryl. The patient was hospitalized for 6 days with no complications. She was started on a high dose of norethisterone for 3 months to block menstruation and allow proper uterine healing.
Results
The patient's postoperative course was uneventful with normal resumption of vaginal menstruation after stopping hormone therapy. After stopping this hormone on June 11, 2012, the patient resumed having unremarkable menstruation vaginally.
Discussion
Frequency
Uterine fistulas are most often uterovesical and uterocolonic. 2 Yet, the uterocutaneous fistula is an extremely rare clinical entity. Although its incidence is not well known, it was noted that about 120 cases of uterocutaneous fistula have been reported in the world literature over the past 200 years. 3 This frequency is probably largely underestimated, because it is known that in developing countries, most of the complications of the uterine and pelvic surgery and of the postpartum period are still not published. This report represents the first documented case of postmyomectomy uterocutaneous fistula observed in the Côte d'Ivoire.
Etiopathogenesis
From the mechanism viewpoint, spontaneous uterocutaneous fistula is extremely rare. There is an intricate mechanism resulting from trauma or inflammation and infection that weakens and destroys the continuity of tissues involved; etiological factors are surgical, obstetric, infectious, and tumor related. The majority of fistulas reported in the literature usually result from postoperative complications of classical cesarean section.2–5 The fistulas may also complicate other pelvic surgeries. 1 Many previous abdominal operations, long maintenance of drains in the abdomen, overlooked intra-abdominal fields, uterine suture with nonabsorbable material, incomplete closure of the uterine incision during cesarean section, and postoperative sepsis are risk factors for formation of these fistulas. Uterocutaneous fistula may be observed in the postpartum period secondary to a difficult and complicated delivery, often after forceps application.
Clandestine and septic abortions and migration of an intrauterine device have been discussed in the literature. 6 Some infectious diseases and tumors resulting from genital tuberculosis and endometriosis have also been identified as etiologic factors for the development of uterocutaneous fistulas.7,8 Ruptured appendix associated with Crohn's disease during pregnancy has been implicated in the study by Baggish et al. 3 Another case of uterocutaneous fistula described in the literature was secondary to an abscess caused by a placenta left in situ after an abdominal pregnancy. 9
With respect to the observations presented here, the risk factors for uteroparietal fistula in this patient were many incisions on the uterus after opening the uterine cavity during myomectomy, and an irregular suture in some places because of many uterine incisions associated with severe postoperative parietal suppuration.
Diagnosis
The reasons for consultation were amenorrhea (absence of menstruation) associated with pelvic bleeding during menstrual period, with bleeding often lasting as long as amenorrhea.2,5 This may also involve postoperative cyclical pelvic bleeding (location on the scar) at the same time as vaginal menstruation1,3 as in the authors' observation. Other more complex signs may exist. 3 The discovery can be fortuitous during an HSG performed, for example, during an examination for fertility. Physical examination generally yields poor results, showing an opening sinus on the surgical skin scar at the site of the pelvic bleeding (Fig. 1).
The demonstration of the fistula was based on the intracervical injection of methylene blue, which is seen coming through the abdominal scar site and on HSG, which demonstrates the fistulous tract (Fig. 2). In some cases, a computed tomography scan and magnetic resonance imaging combined with hysteroscopy may be required for the diagnosis.7,9
Treatment
The spontaneous healing of a uterocutaneous fistula is possible but rare. 3 Uterocutaneous fistulas usually are treated surgically by laparotomy. After careful dissection and adhesiolysis of the uterus to the anterior abdominal wall, the fistula is laid bare and excised according to the fistulous tract, followed by surgical suture of the uterus.1,3–10 If a subsequent pregnancy is not desired or if local conditions do not allow conservative treatment, then hysterectomy can be considered.3–5 Some practitioners have made treated uterocutaneous fistula successfully with gonadotropin-releasing hormone (GnRH) agonists.4,10
In this case, access to GnRH-agonists was expensive and difficult, which is why the medical treatment had been not attempted; also, laparoscopic surgery is, unfortunately, still a “luxury” treatment. Therefore, a laparotomy was performed in this patient. Intraoperatively, the uterus was healthy outside the fistula; uterine conservation (excision of the fistulous tract+uterine suture) was decided on for this young nulliparous woman who strongly desired to be able to have children. The patient was started on hormonal treatment (norethisterone) to suppress menstruation for 3 months to allow good uterine scarring.
Conclusions
Uterocutaneous fistula is an unexpected and very unusual myomectomy sequel. Although medical and conservative surgical treatment is mostly successful, the best treatment must remain prevention based on a better uterine surgery technique, prevention of postoperative infection, and also good control of certain obstetric procedures.
Footnotes
Disclosure Statement
No competing financial interests exist.