
Abstract
Abstract
Introduction
Well-differentiated liposarcoma shows no potential for metastasis unless it undergoes dedifferentiation. The apparently confused terminology derives from the sites of origin of the tumor. When the lesion arises in locations such as the limbs and trunk, wide excision with free margins is curative. In these instances, the term “sarcoma” is not appropriate; hence the term “atypical lipomatous tumor.” However, in locations such as the retroperitoneum and mediastinum, it is usually impossible to obtain a wide surgical excision margin, and, in such cases, local repeated and ultimately uncontrolled recurrence is almost inevitable and often leads to death, even in the absence of dedifferentiation and metastasis. In these situations, the term “well-differentiated liposarcoma” is justified.
ALT/WL identical, both morphologically and karyotypically, and in terms of biologic potential. 3
Liposarcoma of the broad ligament is exceptionally rare. 4 As the tumor described by Singh et al. was of myxoid type, 4 there have been no reports in the literature of ALT/WL in this site.
The first case of broad ligament ALT/WL, which occurred in a patient with endometrial adenocarcinoma, is reported.
Case
A 57-year-old, nulliparous, postmenopausal woman with an unremarkable medical history presented with uterine bleeding. An enlarged uterus was detected during pelvic examination. Transvaginal ultrasound showed an endometrial thickness of 17 mm. At the left side of the uterus, a mass of 80 mm, compatible with a fibroid, was present. Serum level of CA 19.9 was 119 U/mL (normal range 0–37 U/mL). The patient was not under hormonal therapy.
Magnetic resonance imaging (MRI) axial contrast-enhanced T1-weighted image showed a partially encapsulated heterogeneous, predominantly high-signal mass with multiple ill-defined, low-signal areas compatible with septa (Fig. 1). Pelvic lymph node involvement was not detected.
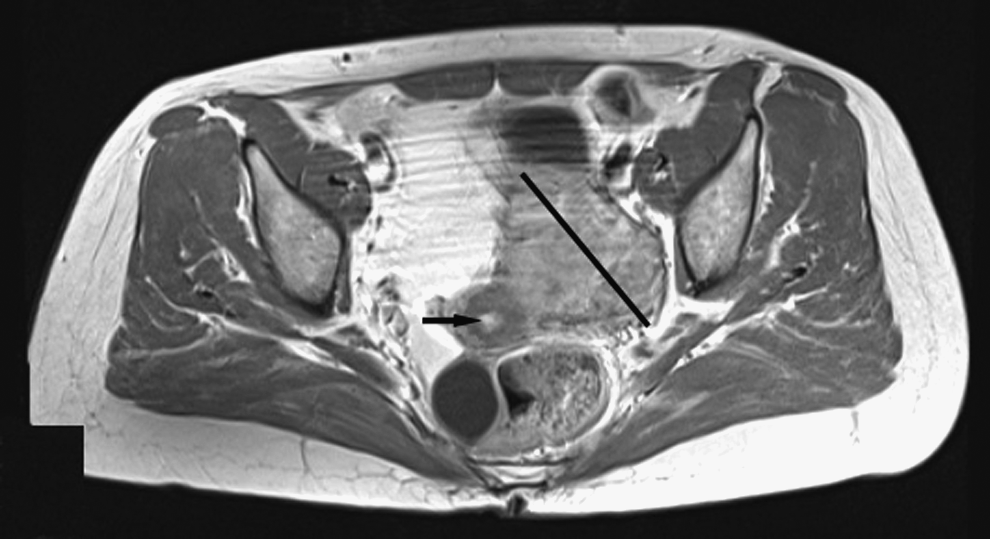
A heterogeneous partially encapsulated mass was detected by magnetic resonance imaging. Arrow indicates the endometrial cavity. The line indicates the parauterine mass.
Office-based hysteroscopic biopsy showed an endometrioid endometrial adenocarcinoma.
At explorative laparotomy, a tumor of 100×80×35 mm arising from the broad ligament was inspected. Total abdominal hysterectomy, with bilateral salpingo-oophorectomy and full pelvic lymphadenectomy, without para-aortic lymphadenectomy, were performed. Endometrium showed a polypoid, white-gray neoplasm. No other abnormalities were noted in the cervix, adnexa, or pelvic cavity.
Results
Macroscopic examination revealed a yellow to white well-circumscribed encapsulated mass.
Histopathologic analysis showed a lipomatous neoplasm, containing fibrous septa, with variation in adipocyte size (Fig. 2A). There was nuclear atypia and hyperchromasia. The fibrous septa contained more hyperchromatic stromal cells (Fig. 2B). There were monovacuolated and multivacuolated lipoblasts (Fig. 2C). There was no necrosis and/or hemorrhage or mitoses.

The endometrium showed an endometrioid adenocarcinoma (grade 2), infiltrating less than half of the myometrial thickness (International Federation of Gynecology and Obstetrics [FIGO] stage IA). The cervix, adnexa, and pelvic lymph nodes were unremarkable.
Discussion
Liposarcoma of the broad ligament is extremely rare. In the literature, only 1 case of myxoid liposarcoma has been reported, 4 and this is the first case of ALT/WL of the broad ligament. The patient came to clinical attention because of uterine bleeding, which was a symptom of underlying endometrial cancer.
As the morphologic features of ALT/WL are quite typical, differential diagnosis with other sarcomas and aggressive angiomyxoma is straightforward. Although the neoplasm was extensively sampled, no carcinomatous elements were detected. Therefore, the diagnosis of malignant mixed Mullerian tumor with liposarcomatous differentiation was ruled out.
ALT/WL in deep anatomical sites tend to recur repeatedly, and may reappear as a dedifferentiated tumor and metastasize. The mortality range for well-differentiated liposarcomas occurring in the retroperitoneum is >80% if the patients are followed up for 10–20 years. 3 Apart from dedifferentiation and metastasis, the incomplete surgical excision causes frequent and repeated recurrences, which lead to death as a result of uncontrolled growth and destructive local infiltration.
In one report of 7 cases of uterine liposarcoma with a follow-up period from 6 to 36 months, 3 cases, all pleomorphic, presented recurrences. 5
In this case, the tumor was totally separated from the uterus and arose within the leaves of the broad ligament and, therefore, could not be labelled as a uterine liposarcoma. The tumor margins were free. There are no previous reports of ALT/WL of the broad ligament; therefore, the risk of dedifferentiation/metastasis is unknown.
Conclusions
This ALT/WL was detected because of the presence of a concomitant endometrial adenocarcinoma. Pathologists should be aware of the possibility of occurrence of this tumor in uterine ligaments and exclude a malignant mixed Müllerian neoplasm. Surgeons should consider that parauterine lipomatous tumors could potentially represent soft-tissue liposarcomas and must be approached accordingly. In order to avoid recurrences, dedifferentiation and eventual distant metastases, surgical resection margins have to be clear.
Footnotes
Disclosure Statement
No competing financial interests exist.