
Abstract
Abstract
Introduction
Case
A healthy 24-year-old primigravida patient at 40 weeks plus 3 days of gestation presented to the hospital in spontaneous active labor. She progressed to complete cervical dilation, with the vertex at +2 station. During pushing, the fetal monitor showed prolonged decelerations with a nadir of 60 beats per minute. Vacuum delivery was attempted unsuccessfully, and the patient was taken to the operating room for an emergent primary cesarean delivery. A Pfannenstiel skin incision was performed, and a low transverse incision was made above the vesicouterine reflection and bluntly extended. The fetus was in occiput posterior position and deeply engaged in the pelvis, complicating infant head extraction. Assistance from below via a vaginal hand was required to elevate the head. Several unsuccessful attempts at delivery were made, and the hysterotomy was extended, with delivery of a male infant, birth weight 3030 g with Apgar scores of 4, 6, and 8 at 1, 5, and 10 minutes. Following delivery, it was noted that the uterus and cervix were completely detached from the vagina circumferentially; however, bilateral uterine vascular supply remained intact, and the uterus appeared well vascularized (Fig. 1). After the hysterotomy was closed, the uterus was reattached to the vaginal cuff with #1 VICRYL™ interrupted sutures. At procedure completion, the patient had an estimated blood loss of 2 L, and had received 3 L of intravenous (IV) fluids and 2 units of packed red blood cells given intraoperatively.
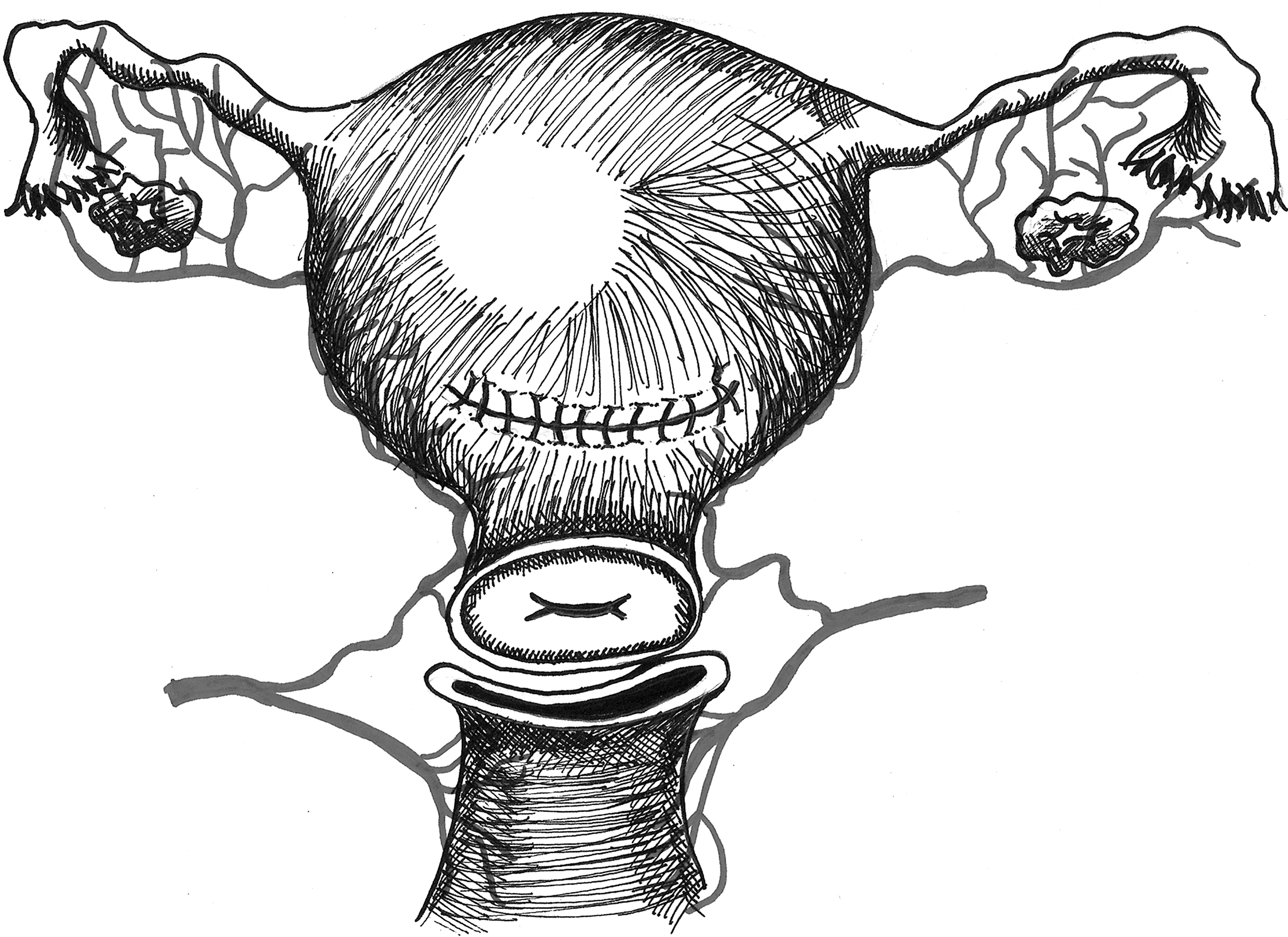
The circumferential tearing of the vaginal vault separating the cervix and vagina with a preserved uterine arterial supply.
Results
The patient's postoperative course was complicated by postoperative endometritis requiring IV antibiotics, and symptomatic anemia requiring additional blood product repletion of 2 units of packed red blood cells and 1 unit of fresh frozen plasma. She was discharged home on postoperative day 4. Speculum examination at her 6 week follow-up clinic visit revealed a well-healed vaginal vault and complete restoration of normal pelvic anatomy.
The neonate required attention in the intensive care unit for respiratory distress and initial suspicion of sepsis, and hyperbilirubinemia requiring phototherapy. He was discharged from the hospital at 6 days of age. Following discharge, he was found to be healthy at a 2 week postpartum visit.
Discussion
This case represents the first description of a rare complication of cesarean delivery in the second stage of labor. Complete separation of the uterus from the vaginal vault with preservation of the uterine blood supply was successfully repaired with surgical restoration of normal anatomy, and peripartum hysterectomy was avoided, reducing morbidity to the patient and allowing the potential for future fertility. Bergholt et al. determined that the preoperative risk factors most highly associated with intraoperative laceration during cesarean section were high birth weight (>4000 g) and low station of the fetus. The authors concluded that these factors likely contributed to a difficult extraction of the fetal presentation through the uterine incision. 1 Approximately 1.5% of cesarean deliveries are complicated by an impacted fetal head, traditionally addressed with the “push” method of assistance with a vaginal hand, or the “pull” method, accomplished by locating the infant legs and performing a footling breech extraction. 2 A prospective, randomized trial by Fasubaa et al. concluded that the “push” method results in higher rates of maternal morbidity, indicated by increased blood loss, greater rates of uterine incision extension and endometritis, and longer operation times and hospital stays, when compared with the “pull” method. 3 Chopra et al. noted more frequent uterine incision extension among those who underwent the “push” method, which they attributed to force from the vaginal hand; however, they noted that superior extensions of the hysterotomy occurred as well with “reverse breech extraction.” 2 Although studies describe extension of the uterine incision and comment on the risk of force from the vaginal hand, there is no mention in the literature of the creation of a separate vaginal laceration with the “push” technique; however, this is certainly a plausible complication of this technique.
Physiologic changes that occur in the vaginal wall in association with pregnancy provide a possible explanation for the location of uterine detachment. Rahn et al. found that pregnancy is associated with increased resting diameter of the vaginal wall and increased tissue distensibility and decreased vaginal wall strength. 4 These conclusions are further supported by a study by Lowder et al. 5 . Overall, physiologic changes in pregnancy affect the biomechanical properties of the vaginal wall and could predispose that area to damage if trauma or overstretching is encountered. Based on the location of the vaginal hand in the “push” method, the superior portion of the vagina would likely receive the greatest physical stress with the maneuver, and laceration with extension could result in complete separation of the uterus from the vaginal cuff.
Given that the patient desired future fertility and particularly because the uterine vasculature was preserved, it was possible to reattach the uterus and cervix to the vaginal cuff instead of performing a peripartum hysterectomy. Reapproximation of the uterus to the vaginal cuff has been successfully performed in fertility-sparing surgery for cervical cancer; specifically vaginal radical trachelectomy (VRT). 6 The patient's situation was not identical to a VRT, as transection of the cervix was not required; however, a similar surgical technique was used in this patient in an attempt to preserve fertility, with the knowledge that this type of surgical repair was feasible because of experience with VRT. Even with damage to some of the blood supply, collateral blood flow to the gravid uterus is ample, and this type of repair may allow for future pregnancies, avoiding the need for postpartum hysterectomy. 7
Conclusions
Complete separation of vaginal vault from the uterus and cervix is a rare complication of cesarean delivery of a fetus with a deeply engaged vertex, with use of the vaginal hand “push” technique. If future fertility is desired and hemodynamic stability can be attained, particularly when the uterine vasculature is preserved, repair should be attempted. This case demonstrates that conservative treatment with repair of uterine detachment through simple reattachment of the vaginal cuff to restore the anatomy can be a feasible alternative to peripartum hysterectomy.
Footnotes
Disclosure Statement
No competing financial interests exist.