
Abstract
Abstract
Introduction
The authors therefore present what is to the best of their knowledge the first report of laparoscopic management of heterotopic pregnancy in a Nigerian hospital.
Case
A 24-year-old G3, P1011 woman presented at the Wesley Guild Hospital, Ilesha, an arm of the Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife, Nigeria on July 23, 2012 at a gestational age of 13 weeks (calculated from her last menstrual period) with complaints of intermittent right iliac fossa pain of 6 days' duration, but which had become persistent about 12 hours before presentation. There was no associated fever, change in appetite, or change in bowel habit.
Examination revealed an anxious gravida who was not febrile, pale, or jaundiced. Her vital signs were all within normal limits. However, she had marked tenderness in the right iliac fossa with rebound tenderness, but there was no rigidity or guarding. Her uterus was 18 weeks size, which was large for date.
On the basis of these findings, a working diagnosis of right ovarian cyst accident in pregnancy was made and an ultrasound scan was performed. The scan revealed a heterogeneous mass in the right adnexum extending to the pouch of Douglas and measuring 8.3 cm×4.6 cm (LxAP) with both solid and cystic components. The left adnexum was free and a single live fetus was seen in the uterine cavity with crown–rump length measuring 53.7 mm corresponding to 12 weeks gestation. There were also multiple intramural fibroids. The placenta was posterior and the amniotic fluid volume was adequate. The patient was therefore counseled, and her informed consent was obtained for laparoscopy.
An emergency laparoscopy was performed with the patient under general anaesthesia using the Palmer's point Verres needle technique to create CO2 pneumoperitoneum and replacing the Verres needle with a 5-mm port through which a 5-mm 0° laparoscope connected to a camera and light source was inserted. A slow-leaking ampullary ectopic pregnancy was discovered in the right fallopian tube, which was grossly dilated and sausage shaped, with altered blood seen trickling slowly from its phimotic fimbrial end. The gravid uterus, left adnexum, and the other intra-abdominal structures were normal. An 11-mm midline port was subsequently introduced under vision, about 12 cm above the umbilicus for the 10-mm laparoscope, and then another 5-mm secondary port in the right hypochondrion.
The right fallopian tube was grasped and desiccated at about 2 cm from its cornual end using a pair of monopolar Maryland forceps connected to an electrosurgical energy source. The desiccated portion was then divided with laparoscopic scissors, and this process of alternating hemostatic coagulation and cutting was repeated along the entire length of the mesosalpinx to completely excise the right fallopian tube intact.
Tissue retrieval was performed through a curvilinear supraumbilical incision with the aid of an improvised tissue retrieval bag made from the wrist portion of a sterile surgical glove tied at one end with a sterile suture. The secondary ports were then removed under vision and the gas was released. Finally, the laparoscope was removed and all the port wounds were closed by suturing with 2/0 Vicryl. The excised right fallopian tube was sent to the pathology department for histological examination, which revealed some variably sized chorionic villi with a central core of mesenchyme and an outer layer of trophoblastic cells, all within the hemorrhage in the lumen of the fallopian tube, thus confirming tubal ectopic gestation. There was no fetus seen.
Results
Postoperatively, the patient received daily progesterone pessaries for hormonal support until the pregnancy was 16 weeks. She was discharged home on the second postoperative day in stable condition and is currently being followed up in the antenatal clinic. The intrauterine pregnancy has progressed and is at 21 weeks' gestational age at the time of this report (Figs. 1 and 2).

Right ampullary heterotopic gestation.
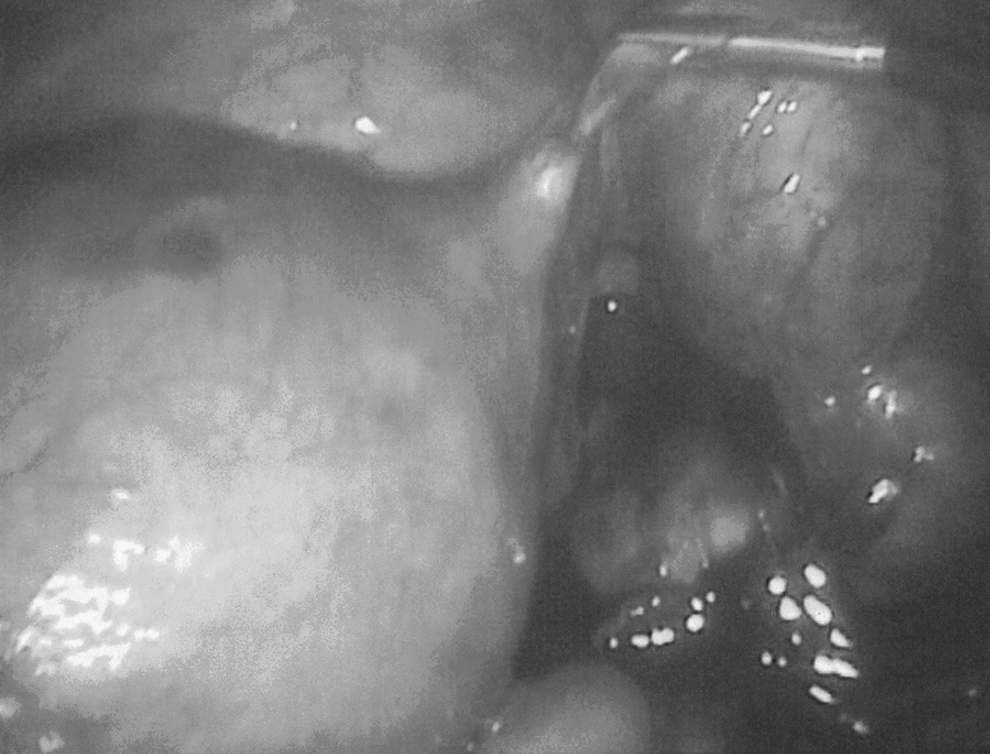
Commencement of laparoscopic salpingectomy.
Discussion
The global incidence of heterotopic pregnancy has risen dramatically, owing largely to the widespread use of assisted reproductive techniques. The fact that heterotopic pregnancy complicates about 1% of all in vitro fertilization pregnancies has made it a considerably anticipated complication of the procedure, thus making the diagnosis less likely to be missed in women undergoing this form of treatment. On the other hand, heterotopic pregnancy in a natural conception such as the patient in this report had is a rare and usually unsuspected condition that often leads to late diagnosis and possible morbidity and mortality. Indeed, in the case presented, the diagnosis was not suspected preoperatively, even though an ultrasound scan had shown a complex adnexal mass coexisting with a normal intrauterine gestation. Given the gestational age of the pregnancy, the presence of cardiac activity within the adnexal mass might have given away the diagnosis, but this was absent in this case because apparently the ectopic pregnancy had failed, resulting in a slow-leaking ectopic gestation.
The incidence of heterotopic pregnancy is derived from the incidence of twin pregnancy and ectopic gestation. 1 Nigeria has one of the highest rates of spontaneous twin gestation in the world as well as a high incidence of ectopic pregnancy. 6 A higher rate of heterotopic pregnancy should therefore not be unexpected. Hence, the need for a very high index of suspicion at all times cannot be overemphasized if avoidable morbidity and mortality from rupture of the ectopic component of a heterotopic pregnancy is to be prevented.
Gynecologic laparoscopy first became available in Ile-Ife in the late 1970s and was used mainly for diagnostic procedures and tubal sterilization. Unfortunately, over the next 2 decades, this rapidly evolving subspecialty in gynecology faltered and eventually came to a halt in the late 1990s as a result of infrastructural decay in Nigerian government hospitals. With the Federal Government's tertiary health care intervention program that was completed in Ile-Ife in 2010 came the fresh supply of some modern video-assisted laparoscopic equipment, which has made operative laparoscopy possible in the authors' medical center.
Apart from the well-established advantages of minimally invasive over open surgery, laparoscopic surgery during pregnancy is also associated with a lower risk of pregnancy loss, as there is less uterine irritation at surgery. 7 Although the presence of a mass such as the 18-week-sized uterus in this case may be considered a relative contraindication to laparoscopy, with proper precautions and modifications to the procedure, laparoscopic surgery can be safely accomplished.
In this case, for example, it was opted to use the Palmer's point 8 rather than the umbilicus for creation of pneumoperitoneum and initial entry, to avoid inadvertent injury to the gravid uterus. After performing the diagnostic procedure using the 5-mm laparoscope through the 5-mm port at the palmer’ point, the authors inserted a midline 11-mm primary port under vision in the epigastric region to be able to achieve a good panoramic view of the uterus and adnexa with a 10-mm laparoscope, and then introduced a second 5-mm working port in the right hypochondrion.
The advanced energy sources such as ligasure and harmonic are not yet available in the authors' medical center. However, it was possible to achieve preventive hemostasis in this case using a simple electrosurgical generator. Similarly, the lack of commercial laparoscopic tissue retrieval bags was overcome through improvisation with the wrist portion of a surgical glove tied at one end with a suture. 9 These and many similar adaptations and improvisations are a necessity, if operative gynecologic laparoscopy is to become an enduring practice in a resource-poor setting such as Nigeria. 10
Conclusions
By and large, it is hoped that this report has illustrated the feasibility of operative gynecologic laparoscopy in a resource-poor setting. Laparoscopy is almost always an option in gynecologic surgery, be it elective or emergency, and the determination of the gynecologist to consider and embrace it even in the face of the numerous prevailing challenges will be pivotal to any progress that will ultimately be recorded in gynecologic laparoscopy in a developing country such as Nigeria.
Footnotes
Disclosure Statement
No competing financial conflicts exist.