
Abstract
Abstract
Introduction
S
This report describes a case of retroperitoneal abscess, which occurred 5 years after laparoscopic sacral colpopexy, and was managed through a vaginal approach.
Case
A 35-year-old Caucasian female patient was referred to the Department of Obstetrics and Gynecology, San Martino Hospital and National Institute for Cancer Research, in June 2010, with a primary complaint of malodorous abnormal vaginal discharge and chronic abdominal pain. In March 2005, at another Institution, she had undergone laparoscopic supracervical hysterectomy and sacral colpopexy for uterine prolapse, which was performed by using an uncoated type 1 monofilament polypropylene mesh and polypropylene monofilament sutures. Her family and past medical histories were unremarkable. She smoked five cigarettes per day. She was not receiving any therapy. She had had two vaginal deliveries. She said that her last postsurgical follow-up had been performed in April 2009, and that no prolapse or mesh erosion had been observed.
She presented to the department of Obstetrics and Gynecology afebrile and in good general condition. During vaginal examination, mesh erosion was observed on the anterior vaginal wall. No prolapse was found. Copious malodorous vaginal discharge was present. The examination with the speculum allowed for identifying the origin of the discharge in the part of anterior vaginal wall where the mesh caused the erosion. Blood, urine, and vaginal cultures were negative. Transvaginal ultrasonography revealed no pathology. Blood parameters were normal. There was no sign of systemic infection (temperature 36.5°C; white blood cell [WBC] 5.82×10,000/mm2; C-reactive protein and erythrocyte sedimentation rate: negative). Empiric intravenous antibiotic therapy with ceftriaxone (1.0 g once a day) was started. The patient underwent magnetic resonance imaging (MRI), which demonstrated a retroperitoneal abscess between the cervix and the posterior bladder wall with a diameter of 3.7×3.2×2.0 cm (Fig. 1). The antibiotic therapy was changed to piperacillin/tazobactam (4.0/0.5 g three times a day).
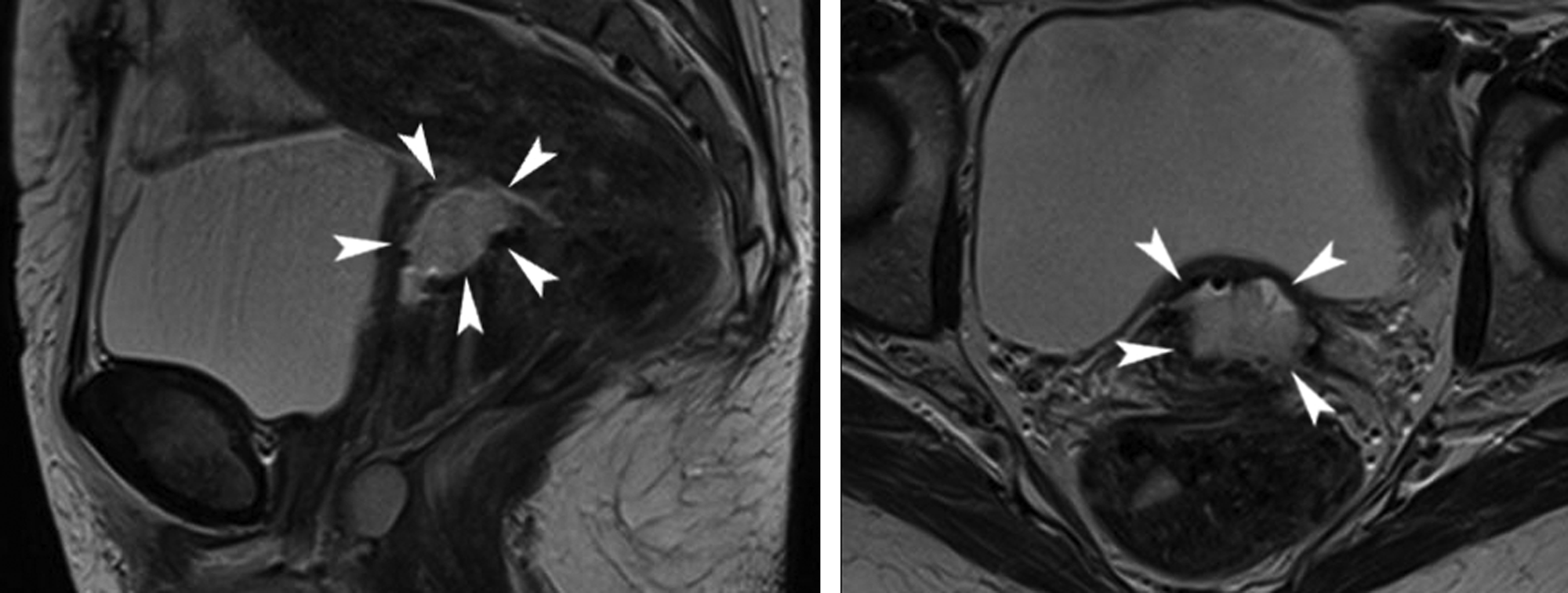
A T2-weighted magnetic resonance imaging (MRI) demonstrates a retroperitoneal abscess located between the cervix and the posterior bladder wall (3.7×3.2×2.0 cm) shown by the arrowheads.
A vaginal approach was chosen to drain the abscess. A colpotomy was performed, and ∼5 mL of purulent fluid was drained. The mesh was still intact, not folded or brunched up in any part. A large portion of the mesh was removed, and the vaginal incision was left open. The culture of the vaginal mesh revealed an extended-spectrum β-lactamase positive carbapenem-sensitive Escherichia coli.
Results
Pain and vaginal discharge disappeared after surgery. The patient was discharged from the hospital in good health 1 week after the operation. Imipenem (1.0 g three times a day) was administered for 3 weeks after surgery. Follow-up visits were performed at 1, 6, and 12 month follow-ups. No recurrence of the abscess was observed. At 1 year follow-up, the patient had stage 1 prolapse of the cervix and anterior vaginal wall according to the pelvic organ prolapse quantification system (POP-Q). She did not complain of any symptom, and no further treatment was required.
Discussion
Despite the fact that sacral colpopexy is an established and reliable operation for apical prolapse treatment, there are potential complications that need to be balanced against its benefits. A great evolution has been made in synthetic mesh; nowadays, the most commonly used synthetic mesh material is the macroporous monofilament. This material permits migration of macrophages and mast cells, to protect from infections. These meshes are more resistant than the fascial tissues of the patients, reduce operative time, and simplify the technique, avoiding fascial harvesting procedures. Mesh erosion is a common complication of the use of synthetic prosthesis in vaginal reconstructive surgery for apical prolapse; it occurs in 2.2% of the patients 1 and can be insidious to manage. The management of vaginal mesh erosion is usually local excision without removing the entire mesh.
Mesh erosion can also involve other locations. Patsner reported a case of mesh erosion into the bladder that presented with hematuria and stone formation. It resolved only when the bladder was opened and the exposed portion of mesh was removed. 4 Different cases of osteomyelitis have been reported.2,3,6,7 Weidner et al. 6 presented 2 cases in which the main complaint was low back pain, and at examination there was no vaginal mesh erosion or abscess; after prolonged antibiotic therapy, resolution of the disease was obtained without removing the mesh. Vaginal mesh erosion was reported in the other three reports. Hart et al. 2 described a case in which a vaginal mesh erosion treated with local excision was followed by the formation of a persistent sinus tract from the vaginal apex to the sacrum, sacral osteomyelitis, and a potentially life-threatening sacral abscess. Because of the potential recurrence of sinus tract formation, the abdominal approach was chosen and suggested by the authors for management of this condition. Another report described the case of a patient who developed vaginal mesh erosion complicated by staphylococcal bacteremia. Complete removal of the mesh and prolonged (3 weeks) intravenous antibiotic therapy did not prevent the onset of osteomyelitis, which caused progressive neurologic symptoms. A decompression laminectomy was finally required to allow the complete recovery and resolution of symptoms. 7 Recently, Collins et al. showed that complications of sacral colpopexy can occur even a long time after surgery. 3 A woman who was treated by posterior colporrhaphy and sacral colpopexy with macroporous polypropylene mesh developed vaginal mesh erosion 3 years later. After local excision of the mesh, its complete removal was scheduled for mesh erosion recurrence. One week before the operation, the patient's chronic back pain became worse and she postponed surgery. She subsequently developed an ascending infection of the second erosion, which led to the development of purulent drainage, back pain, severe infectious complications including an infected thrombus in the inferior vena cava, sacral osteomyelitis, and a complex abscess with pre-sacral and epidural components.
Abscesses are rare complications of sacral colpopexy, but they can have potentially life-threatening infective consequences.
The case reported here differs from those previously reported, as the complications were less serious. The patient was never in a life-threatening condition and she did not present with systemic involvement. However, this report is interesting because the complication occurred a long time after the initial operation. The patient presented to the Department of Obstetrics and Gynecology 63 months after sacral colpopexy. She stated that the last follow-up visit, performed in April 2009, had been normal. When she was examined at the Department of Obstetrics and Gynecology, anterior vaginal mesh erosion was observed and, therefore, it can be hypothesized that it had occurred between 50 and 62 months from the original surgery. This patient had no risk factors for mesh erosion, except for smoking (five cigarettes per day); she was young and did not use immunomodulatory drugs. Furthermore, the she had undergone supracervical hysterectomy, which has been reported to be associated with lower incidence of mesh erosions and infections than concomitant total hysterectomy. 9
Abscesses are usually located in the sacral region.2,3 This is believed to be the first report of an abscess occurring remotely from surgery in a woman who had undergone sacral colpopexy preserving the cervix. The cause of the abscess could be related to an ascending infection from the anterior vaginal wall erosion. Obviously, because of the long interval between surgery and the development of the symptoms, it seems unlikely that the abscess was caused by an intraoperative infection. The location of the abscess was unusual, as it remained circumscribed to the retroperitoneal space between the cervix and the posterior bladder wall. It can be hypothesized that the cervix acted as a barrier in preventing the abscess to extend into the pelvis toward the sacral area.
Based on the position of the abscess, a vaginal approach was chosen because it was less invasive than an abdominal one. Furthermore, the volume of the abscess was moderate, the vital, and the laboratory parameters of the patient were normal without any sign of systemic infection. A strict follow-up was performed to ensure that there was no recurrence or further infective complication. Finally, the patient developed a stage 1 prolapse of the cervix and anterior vaginal wall according to the POP-Q system. It is likely that the removal of a large part of the mesh caused this small prolapse, which was not clinically relevant.
Conclusions
Follow-up is very important in patients undergoing sacral colpopexy. Although remote complications are rare, they may be very serious and potentially life-threatening conditions. However, when patients are satisfied with surgery and their symptoms improve or disappear, they may not have follow-up consultation. A great effort should be made to increase the adherence of patients to postoperative follow-up. Complications should be always managed in the least invasive way, without neglecting the safety of the patient. In this patient, vaginal surgery combined with antibiotic therapy was successful in treating the retroperitoneal abscess.
Footnotes
Disclosure Statement
No competing financial interests exist.