
Abstract
Abstract
Endometriosis is a common and chronic inflammatory disorder affecting 10%–16% of women of reproductive age. Although endometriosis is a benign condition, it has negative effects on the quality of life and fertility of women affected. The annual cost in the United States from endometriosis is estimated at $65 billion, because of lost productivity and medical expenses. The socioeconomic impact of endometriosis is evident; however, effective treatment options elude clinicians. Medical management typically consists of nonsteroidal anti-inflammatory drugs and hormonal drugs that suppress ovarian function. Often, however, medical treatment regimens do not satisfactorily alleviate the intractable pelvic pain and are counterproductive for fertility. When medical treatment is suboptimal for managing endometriosis-related symptoms, complete excision of the deeply infiltrating lesions, endometriomas, and associated scar tissue can significantly alleviate pain and improve fertility. In this review, the current management of deeply infiltrating endometriosis, focusing on the surgical treatment of deeply infiltrating disease in the pelvis, urogenital tract, bowel, diaphragm, and chest, are discussed. (J GYNECOL SURG 29:118)
Introduction
Pathophysiology and Etiology
Endometriosis is defined as ectopic uterine endometrial glands and stroma located on viscera throughout the body, including organs in the pelvis, abdomen, and chest. 4 Although the exact mechanism is unknown, the most accepted theory of its pathogenesis is retrograde menstruation. Sampson's theory suggests that during retrograde menstruation through the Fallopian tubes, some of the menstrual debris attaches to peritoneal surfaces, and invades into the tissue. 5 Implantation of endometrial tissues into the peritoneal wall and other extragenital locations as well as subsequent lesion development and recruitment of other cell types promoting invasion and proliferation leaves many unanswered questions of the basic mechanisms.
Multiple factors may contribute to the development of endometriosis. Although most women are diagnosed between the ages of 25 and 35 years, adolescents who complain of pelvic pain and dyspareunia are commonly found to have endometriosis. In many cases of women <17 years of age, Müllerian anomalies, vaginal obstruction, or imperforate hymen are associated with a higher risk for endometriosis. 6 Women who had in utero exposure to diethylstilbestrol have higher rates of endometriosis because of their inherently higher rates of reproductive tract anomalies. 7 Early menarche, short menstrual cycles, infertility, and diet high in “trans” fat and red meat have also been associated with endometriosis.8,9 Higher parity, lactation, exercise, and diet high in vegetables/fruits and omega-3 fats have been correlated with a decreased risk of endometriosis.10–13
Endometriosis is reported to have a heritable component. 14 Early research regarding endometriosis noted clusters of affected relatives, suggesting a familial occurrence.15,16 In 1980, Simpson et al. published the first formal genetic studies on women with histologically proven endometriosis. 17 In these studies, he found that 6.9% of first-degree relatives had endometriosis; by contrast, <1% of their husbands' female relatives had endometriosis. 17 A follow-up study established a genetic risk of developing endometriosis: 7% for first degree relatives and 2% for second degree relatives. 18 Twin studies have described multiple pairs who are concordant for endometriosis. Concordant twins tended to have moderate or severe disease.19,20 Although there is no established inheritance pattern, higher incidences of the disease within families suggests that endometriosis has a genetic component, and that a predisposition to the disease is inherited as a complex genetic trait for which the phenotype likely reflects interactions between allelic variants and environmental factors.
Clinical Symptoms
Endometriosis exhibits a broad spectrum of clinical signs and symptoms depending upon the sites affected by the disease. The most common locations are the pelvis, where endometriosis implants on the peritoneal surfaces of the uterus, bladder, posterior cul-de-sac, sigmoid colon, and ovaries.21–23 Pain is the most common symptom associated with endometriosis, and is attributed to three mechanisms: 1) direct and indirect effects of focal bleeding from endometriotic implants, 2) actions of inflammatory cytokines in the peritoneal cavity, and 3) direct and two way interaction between lesions and the central nervous system. 24 The pain associated with superficial disease is related to a local inflammatory response caused by cyclic focal bleeding of the peritoneal implants. Pain from deeply infiltrating disease is thought to be a result of endometriotic lesions invading into the nerves of the pelvic floor, causing chronic and intractable pain. Severe dysmenorrhea and deep dyspareunia are associated with DIE of the posterior cul-de-sac and uterosacral ligaments (USL). 25 Women with endometriosis adjacent to or within the rectal wall may complain of dyschezia. 26 However, there is often no direct relationship between pelvic pain and the stage, site, or morphologic characteristics of endometriosis.26–28
Endometriosis is also strongly associated with infertility or subfertility. The overall prevalence of endometriosis is greater in infertile than in fertile women. 29 Among women who were treated with assisted reproductive technology in 2009, live birth rates for women with endometriosis (35.3%) were comparable to those for women diagnosed with tubal factor (32.3%), male factor (37.6%), and unexplained infertility (33.7%). 29 The theorized cause of infertility is 1) anatomical distortions of the adnexa that inhibit or prevent ovum capture after ovulation, and 2) excess production of inflammatory prostaglandins, metalloproteinases, cytokines, and chemokines, which impair ovarian, tubal, and endometrial function. 30
Diagnosis
Laparoscopic visualization and histologic confirmation via biopsy of suspected lesions assist in confirming the diagnosis of endometriosis. Visual identification alone results in a high false-positive rate.31,32 To standardize the extent of disease, endometriosis is classified into four stages by the American Society for Reproductive Medicine scoring system, which was revised in 1996. 33 A point system based on the quantity and location of endometriosis lesions, density of adhesions, and amount of scarring, ranks the disease into stage I (minimal), stage II (mild), stage III (moderate), and stage IV (severe) disease.
Two subtypes of endometriosis are differentiated by gross and microscopic inspection: superficial endometriotic implants and deeply infiltrating endometriosis (DIE). Superficial endometriotic implants are shallow, <5 mm in depth, and typically scattered throughout the abdominal-pelvic peritoneal surfaces. Its characteristic histology is described as deposits of endometrial-like glands and stroma with evidence of menstrual shedding. A second manifestation is the deeply infiltrating type in which the endometriotic lesion infiltrates >5 mm beneath the peritoneum. 34 These lesions show marked fibrosis and smooth muscle hyperplasia in addition to the classical combination of endometrial glands and stroma. 35 DIE can cause not only severe dysmenorrhea, but also significant nonmenstrual pain, dyspareunia, dysuria, and dyschezia. 36 Although the amount of pain is not often correlated with the extent of superficial endometriosis or its location, 28 DIE of the vagina, posterior cul-de-sac, and adnexa are significantly related to the severity of dysmenorrhea. 37 Patients with DIE are also reported to have a positive family history of endometriosis, a higher incidence of combined oral contraceptives (COC) use for primary dysmenorrhea before 18 years of age, and longer duration of COC use. 38
Medical Management of Endometriosis
A main principle of treating endometriosis is symptom management, focusing on the relief of endometriosis-related pain. NSAIDs are recommended as first-line therapy in combination with COC for women with known or suspected endometriosis. 39 Use of COC results in ovulation inhibition, decreased gonadotropin levels, reduced menstrual debris, and decidualization of endometriotic implants. 40 Extended-cycle COC eliminate the dysmenorrhea-associated withdrawal bleeding. A 2 year, prospective, clinical trial of women with endometriosis-associated dysmenorrhea unresponsive to previous cyclic COC treatment found that continuous administration of COC provided significant pain reduction from baseline levels (p<0.001). 41
Progestins are another class of drugs used for the treatment of endometriosis. They suppress the hypothalamic–pituitary–ovarian axis, induce anovulation, and reduce serum estrogen levels, causing atrophy of both the eutopic endometrium and endometriotic lesions.42,43 Progestins are available in many forms including pills, injectable solutions, subdermal implants, and intrauterine devices. Oral norethindrone acetate and subcutaneous depot medroxyprogesterone acetate (DMPA) have been approved by the United States Food and Drug Administration for treatment of endometriosis-associated pain. Two randomized control trials have shown that DMPA was equivalent to GnRH agonist in reducing pain, with significantly less bone loss.44,45 A 6 month, prospective, observational study of the levonorgestrel intrauterine system showed significant improvement in the severity and frequency of pain and menstrual symptoms in women with minimal to moderate endometriosis. 46
For women who fail therapy with NSAID and COC and/or progestins, therapy with a GnRH agonist is appropriate. GnRH agonists stimulate pituitary GnRH receptors and interrupt the normal pulsatile stimulation. The gonadotropins, luteinizing hormone, and follicle stimulating hormone, are downregulated, leading to hypogonadism and reduction in estradiol. GnRH agonists are approved and highly effective for treating endometriosis-associated pain. 47 They do have considerable side effects including vasomotor symptoms, vaginal dryness, and osteopenia. GnRH agonist-induced osteopenia is reversible with short-term use (3 or 6 months), but may not be with long-term use or with multiple cycles. GnRH therapy can be used off label for longer periods, but should be used in combination with add-back therapy. Daily norethindrone 5 mg with or without a low-dose conjugated estrogen can decrease the negative side effects of GnRH agonists without sacrificing efficacy. 48
Danazol is a synthetic androgen and the first drug approved to treat endometriosis-associated pain. The drug inhibits ovarian steroidogenesis, resulting in a decreased secretion of estradiol and an increase of androgens. 49 Although highly effective in reducing pain, it has undesirable, masculinizing side effects that include acne, hirsuitism, and myalgias. 50 Consequently, danazol is rarely prescribed, in favor of GnRH agonists that are equally effective.
Surgical Management of DIE
Although the first-line management of endometriosis is medical therapy, in many cases medical management does not alleviate the endometriosis-associated pain symptoms caused by inflammation and scarring. In these circumstances, surgical excision of the DIE may be necessary to remove the endometriosis and scar tissue, restore anatomy, and prevent recurrence.
Previously, hysterectomy and bilateral salpingo-oophorectomy were considered the standard treatment of endometriosis, and they were performed via laparotomy. However, surgery for endometriosis has evolved into a minimally invasive and targeted procedure. Pivotal in this transformation was the introduction of video-assisted endoscopy developed by Nezhat, who revolutionized the surgical management of endometriosis. 51 The ability and efficacy to laparoscopically manage DIE involving the bladder, ureter, bowel, diaphragm, para-aortic lymph node dissection, radical hysterectomy, vesicovaginal fistula, rectovaginal fistula, ovarian remnant, sacral colpopexy, repair of major vessels, and laparoscopy during advanced pregnancy were established in the late 1980s and early 1990s.52–59 Laparoscopic treatment of DIE is becoming the standard of care, and is preferable to laparotomy, but may be limited by the skill and expertise of the surgeon, and the availability of proper instruments. 60
Ovarian endometriomas
Management of endometriomas is controversial, because of concerns over removing too much normal ovarian stroma and balancing the risks of endometrioma recurrence if lesions are incompletely excised. Endometriomas have been treated with wedge resection, enucleation (stripping the cyst wall from the ovarian cortex), and drainage with and without ablation of the internal cyst wall. An argument for simple drainage and cyst wall ablation is that the histologic analysis of the endometrioma cyst wall shows that endometriosis is present in 10%–90% of the cyst surface (median 60%) but usually does not penetrate more deeply than 2.0 mm. 61 Therefore, ablation should destroy the lesions because of their shallow depth. However, a Cochrane review concluded that enucleation of an endometrioma compared with coagulation or laser vaporization was associated with a lower rate of recurrence of the endometrioma, reduced pelvic pain, and increased pregnancy rate in women who previously had been infertile. 62 Two randomized clinical trials included in the Cochrane review have shown that endometriotic cyst excision is associated with higher spontaneous pregnancy rates than are other surgical techniques.63,64
The enucleation technique for cystectomy may remove a significant proportion of normal and functional ovarian tissue. A nonrandomized retrospective study in 28 infertile patients, who underwent laparoscopic cystectomy for endometriotic cysts <4 cm, demonstrated a diminished ovulatory rate in the operated ovary from 41% to 19%. 65 The risk of ovarian failure after excision of bilateral ovarian endometriomas is ∼2.5%. 66 Nevertheless, current evidence-based research favors the enucleation technique, because of the lower risk of recurrence, alleviation of pain symptoms, and improvement of fertility.
Endometriosis of the USL
DIE of the uterosacral ligaments (USL) is found in up to 70% of all women with endometriosis.4,67 Scarring and inflammation of the USL are typically accompanied by substantial endometriotic lesions involving the rectosigmoid, posterior cul-de-sac, and vagina. At the time of laparoscopic diagnosis, resection of endometriotic lesions and scar tissue is recommended. In addition to alleviation of endometriosis-related pain symptoms, fertility appears to be improved for all stages of endometriosis after laparoscopic lysis, coagulation of superficial lesions, and resection of deeply infiltrating lesions of the USLs. 68
For women with severe and unmanageable pelvic pain, two neurectomy procedures have been studied for the management of chronic pelvic pain: the laparoscopic uterosacral nerve ablation (LUNA) and the presacral neurectomy (PSN). The LUNA procedure involves the transection of the USLs at their intersection into the cervix. The PSN procedure consists of the complete surgical removal of the presacral nerves lying within the boundaries of the interiliac triangle. Both neurectomies aim to interrupt the majority of sensory nerve fibers, diminishing pain. A Cochrane analysis of LUNA and PSN reported that for primary dysmenorrhea, LUNA was more effective than control or no treatment at 12 months (odds ratio [OR] 6.12; 95% confidence interval [CI] 1.78–21.03), and LUNA was as effective as PSN for short-term pain control, but PSN was shown to be significantly more effective at 12 months (OR 0.10; 95% CI 0.03–0.32). 69 Several randomized trials failed to demonstrate efficacy for LUNA procedure in the treatment of chronic pain. 70 In addition, several complications after the LUNA procedure have been reported, including uterine prolapse 71 and bladder dysfunction, particularly voiding dysfunction with reduced sensation and areflexia. 72 PSN for the treatment of midline pelvic pain has been shown to provide significant symptom relief.69,73 Complications of PSN are rare, but may include constipation, because of the transection of the parasympathetic fibers that stimulate evacuation of the rectosigmoid. Some women have also reported altered bladder sensation caused by interruption of sympathetic bladder fibers.
DIE of the rectum
Women with severe endometriosis commonly have deeply infiltrating disease involving the rectum (DIER). In a series of 51 women with stage 4 disease involving the bowel, 87% of the preoperative symptoms of dysmenorrhea (85.3%), dyspareunia (55.9%), rectal pain (41.2%), constipation (44.1%), rectal bleeding (14.7%), bloating (29.4%), and tenesmus (8.8%) were alleviated with radical surgery. In this series, management of bowel endometriosis included superficial excision or shaving of the nodule (n=26), bowel resection (n=8), and full thickness disc excision (n=5). Four postoperative complications occurred overall: pyosalpinx (n=1), anastomotic leak with pelvic abscess (n=1), antibiotic-associated diarrhea (n=1), and pneumonia (n=1). Two postoperative complications occurred in the segmental resection group, 1 complication in the superficial excision group, and 1 complication in the group with resection not involving the bowel. 74 Most colorectal surgeons prefer segmental colorectal resection for the treatment of DIER. Their argument is supported by retrospective studies reporting significant improvement in pain and quality of life, and lower risk of recurrence.75,76 Radical resection of the endometriosis is believed to prevent the risk of recurrence, 77 and their treatment decision is supported by studies showing that disc excision does not lead to the removal of microscopic satellite endometriotic lesions around the primary nodule. 78 Nodule excision is another surgical approach to DIER that has fewer postoperative complications and less of the unpleasant digestive and urinary dysfunction that results from partial removal of the rectum.79,80 However, both disc excision and superficial shaving techniques may leave microscopic endometriotic lesions outside the visible lesion and fibrous scarring. With respect to reproductive performance, a cohort of 105 women with rectovaginal endometriosis underwent conservative surgery versus expectant management. There was no statistical difference in pregnancy rates between the two groups (15 out of 44 women who chose surgical management became pregnant versus 22 out of 61 women who chose conservative management). There was a significant difference in the pain-free interval for women who had surgical management. 81
DIE of the small bowel, large bowel, and appendix
DIE involving the bowel (Fig. 1) affects ∼10%–12% of women diagnosed with endometriosis.4,82 Mohr et al. reported a series of 187 women with endometriosis involving the bowel, and the most common symptoms were pelvic pain 99%, dyschezia 74%, back pain 55%, constipation 74%, diarrhea 41%, melena 16%, and nausea 8%. 83 The surgical treatment dilemma for endometriosis of the small bowel, similar to management of the colon and rectum, is whether to shave the lesion from the surface of the bowel, excise a disc of bowel wall around the endometriosis, or resect a segment of bowel. A retrospective study compared women undergoing different surgical procedures for removal of deeply infiltrating bowel endometriosis. Complete pain relief in the immediate postoperative period was significantly more likely with partial bowel resection than with shaving only, 92% versus 80% (p<0.04). However, shaving the endometriotic lesions was associated with a significantly lower complication rate: 6%, compared with 23% for disc excision (p<0.007) and 38% for segmental resection (p<0.001). 83 A prospective study of 500 young women demonstrated that the shaving technique preserved organs, nerves, and blood vessels, and resulted in high pregnancy rates, low complication rates, and few recurrences. 84 Therefore, shaving or disc excision is preferable in women of reproductive age, except when the bowel lumen is compromised or when a segment of bowel is extensively involved with endometriosis and requires multiple shavings or disc excisions.
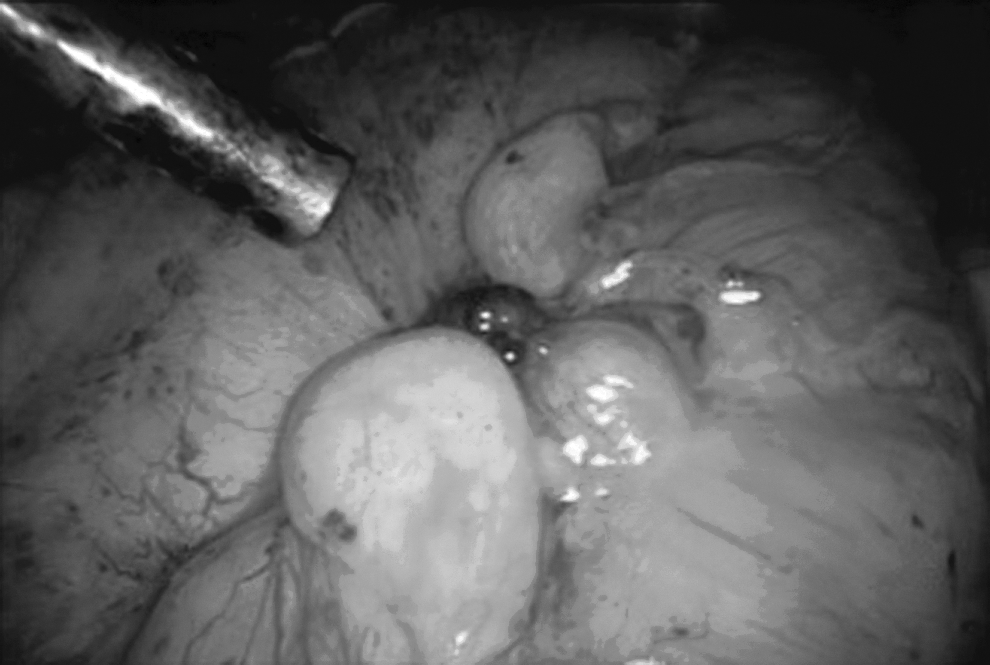
Deeply infiltrating endometriosis of the sigmoid colon (center) with puckering. Lesions of the colon and rectum can cause symptoms of constipation, tenesmus, bloating, rectal pain, and rectal bleeding.
The prevalence of endometriosis of the appendix is reported to be ∼2.8% based on a case series by Gustofson et al. In this study of a group of 133 women undergoing laparoscopy for chronic pelvic pain, 97 women (72.9%) had biopsy-proven endometriosis, but only 4 (2.8%) had endometriosis of the appendix. 85 However, in a series of 231 women who had an appendectomy during laparoscopic surgery for chronic pelvic pain in conjunction with endometriosis, concomitant pathology was discovered in 115 (47.8%). 86 Endometriosis of the appendix can present with symptoms similar to acute or chronic appendicitis, cyclic melena, lower intestinal hemorrhage, and intestinal perforation. Recommended treatment for endometriosis of the appendix is appendectomy.
Urinary tract endometriosis
Urinary tract involvement occurs in 1%–2% women with endometriosis. 87 The bladder is the most common site. Symptoms that suggest bladder endometriosis are dysuria, urinary frequency, menouria, and cyclical urethral as well as chronic pelvic pain.87,88 Cystoscopy can assist in the diagnosis of bladder endometriosis (Fig. 2) through histologically confirmed biopsy of suspected lesions. However, transurethral resection of lesions involving the bladder wall and tissue surrounding the bladder is not recommended, because of the possibility of bladder perforation and subsequent injury to adjacent organs. It is preferable and recommended to resect DIE of the bladder laparoscopically.56,89 In a series of 15 women with DIE of the bladder, lesions were located on the dome in 8 women and on the trigone in 7 women. All of the women underwent laparoscopic full-thickness segmental resection with single layer closure of the bladder without significant perioperative complications. A Foley catheter was left intact for 10–14 days, and the women had a postoperative cystogram 7–14 days after the procedure, with removal of the Foley catheter. Two of 15 patients had extravasation on cystogram without peritoneal spillage. 87

Cystoscopic view of transmural endometriosis of the bladder. The dark-colored endometriotic lesions (arrow) proliferated through the bladder wall into the bladder mucosa.
Endometriosis involving the ureters (Fig. 3) occurs in 15%–20% of urinary tract cases, and of these cases, bilateral disease occurs in 20%–25%. Most commonly it affects the distal ureter, less commonly it affects the mid ureter, and it rarely affects the proximal ureter. 90 Endometriosis extrinsically encases the ureters, causing ureteral strictures and hydronephrosis. 91 Symptoms of ureteral disease include flank pain, cystitis-like pain, and pelvic discomfort. 92 If renal function is normal with minimal hydronephrosis, then hormonal treatment with a GnRH agonist may be prescribed for 6–9 months. 93 Obstructive uropathy is better managed first surgically, then with a course of postoperative GnRH agonist. 91 However, women with ureteral endometriosis may have silent loss of renal function without any genitourinary symptoms. 94 The choice of treatment of ureteral endometriosis depends upon the location and extent of disease. In a series of 30 women with ureteral endometriosis, laparoscopic ureterolysis was performed in 22 of 30 women (73.3%), segmental ureteral resection and ureteroureterostomy was performed in 5 women (16.7%), and ureterectomy and ureteroneocystostomy was performed in 3 women (10%). 95 In this series, infiltrative ureteral endometriosis was managed with segmental resection of the diseased ureter and subsequent ureteroureterostomy or ureteroneocystostomy depending upon the location and length of the remaining ureter. 95 A larger case series of 96 women all underwent ureterolysis with endometriotic excision or ablation. Two women had resection and ureteroneocystostomy with a psoas hitch, because of extensive involvement and obstruction of the distal ureter. Six patients had Double-J® stents placed after extensive ureterolysis. 96 A postoperative course of COC or GnRH agonist is recommended to lengthen the interval between disease recurrences.
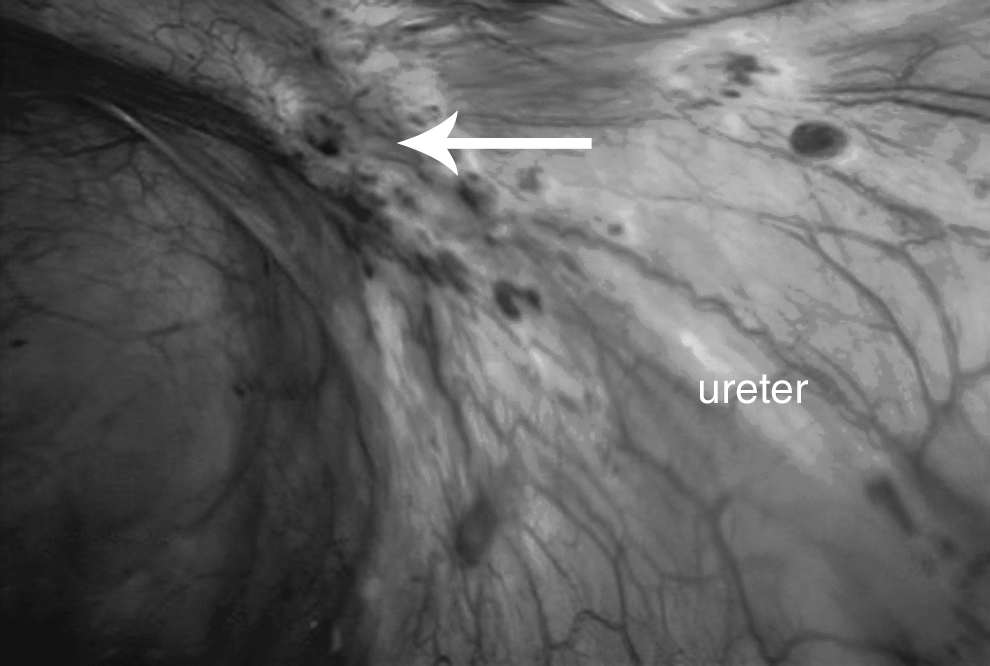
Endometriosis over the right ureter and pelvic sidewall. The lesions attached to the peritoneum over the right ureter (arrow) have invaded into the pelvic sidewall. The location and scarring caused by endometriosis can result in hydroureter, hydronephrosis, and silent loss of renal function.
Endometriosis of the abdominal wall
Abdominal wall endometriomas (AWE) are uncommon, and occur as a secondary process in surgical scars. In a retrospective review, 64 cases were identified at a tertiary referral center during a 20 year period. 97 Sixty-two women had abdominal surgery (61 cesarean sections and 1 appendectomy), and 2 women had umbilical endometriosis and no previous history of surgery. The most common complaint was a tender mass, which enlarged and became more symptomatic during menstruation. Fifty-six women had cyclic pain, 5 had chronic pain, 3 had an asymptomatic mass in a surgical scar, and 2 had cyclic drainage and bleeding from surgical scar endometriosis. Sixty-two women were treated with wide local excision of the lesion that involved the fascia in 53 cases, rectus muscle in 21 cases, and peritoneum in 10 cases. The mean diameter of the AWE was 3.1 cm (range, 1–15 cm). Two patients required synthetic graft for the large fascial defect. Two women declined surgical management and underwent hormonal therapy until menopause. Five women who underwent surgical excision had recurrences, and 1 progressed from atypical endometriosis to sarcoma during the follow-up period. Wide local excision with clear margins is the recommended treatment for AWE. Surgical excision should include at least 5 mm of surrounding healthy tissue, and care should be taken to avoid rupture of the mass and reseeding of the endometriosis.
Perineal endometriosis
Endometriosis can develop in the perineum, most often occurring after vaginal delivery. The prevalence of perineal endometriosis was 0.31% (36 of 11,487) among women surgically treated for pelvic and extragenital endometriosis at a large university hospital. 98 Twelve women had endometriosis at perineal laceration sites, and 24 had lesions at episiotomy scars. Symptoms included perineal lesions that cyclically increased in size and tenderness during menses. In this series, complete surgical excision of the lesions with or without hormonal treatment resulted in no recurrences of the perineal endometriosis. However, incomplete excision of the endometriotic lesions even with postoperative hormonal therapy resulted in perineal recurrence in 7 of 7 women. Incomplete excision was the result of the close proximity of the lesion to the anal sphincter.
In a different case series of 31 women with perineal endometriosis involving the anal sphincter, all had a history of vaginal delivery with perineal trauma. In 20 (64.5%) women, the endometriotic lesion occurred at the episiotomy site, and in 11 (35.5%) women the lesions occurred at the site of perineal laceration. Complete narrow excision, close to the edge of the endometrioma, with a 0.3–0.5 cm margin, was performed in 30 (96.8%) cases. Average size of the lesion was 2.7 cm (range, 1.5–4 cm). Part of the anal sphincter was excised during surgery, and primary anal sphincter repair used the apposition technique in 29 cases and overlapping technique in 1 case. In 1 case (3.2%), incomplete excision was performed because the perineal lesion was too large (4 cm) to excise completely. Pre- and postoperative hormonal therapy for 3–6 months was given to more than half of the women, including pre- and postoperative DMPA for the patient with incomplete excision. Postoperative complications included 1 perineal abscess, but wound healing was satisfactory in 30 cases, and all had good sphincter control with no anal incontinence during follow-up. There was 1 recurrence in the complete excision group, and the patient with incomplete excision had a recurrence 6 years after her initial surgery. 99
Diaphragm and thoracic endometriosis
Endometriosis located on the diaphragm (Fig. 4) and in the thoracic cavity are rare manifestations and reported in single cases or small case series. Two theories may explain the presence of endometriosis in the chest: the retrograde menstruation theory, in which endometrial tissue migrates via retrograde menstruation into the thorax through diaphragmatic defects, 5 and the microembolization theory, in which sloughed endometrial tissue travels into the parietal pleura and parenchyma. 100 If diaphragmatic endometriosis is found incidentally and the patient is asymptomatic, an expectant approach with no further intervention is recommended, because of the risk of injury to the diaphragm, phrenic nerve, lungs, blood vessels, and heart. 32 However, for those patients who are symptomatic, surgery has proven beneficial when other medical interventions have failed.57,101,102 In a case series of diaphragmatic endometriosis, the most common symptom was catamenial chest pain. All 4 women diagnosed with diaphragm lesions during laparoscopy also had concomitant video-assisted thoracoscopic surgery (VATS) that documented the presence of thoracic endometriosis (TE) defined as endometrial implants on the parenchyma, parietal, and visceral pleura. Therefore, use of thoracoscopy in combination with laparoscopy is recommended to prevent the underdiagnosis and treatment of TE. 103 An analysis of 110 patients with TE found that the most common clinical presentations were pneumothorax (72%), hemoptysis (14%), hemothorax (12%), and lung nodules (2%). The right hemithorax was more often affected (85%) than the left. As expected, the presence of parietal and visceral pleural endometriosis implants were associated with a fivefold increase in hemothorax and parenchymal lung involvement. 104 Both VATS and open thoracotomy permit the exploration of the thoracic cavity, resection of endometriotic implants, closure of diaphragmatic defects, and pleurodesis, if indicated.

Severe endometriosis of the right hemidiaphragm. Multiple dark-colored endometriotic lesions and associated light-colored fibrosis covered the right hemidiaphragm.
Definitive surgery for endometriosis
After conservative surgery for endometriosis, recurrent disease and pain are common, with symptoms returning within months. Often after conservative management, there is a need for additional surgical treatments. 105 Several methods to reduce the return of endometriosis-related symptoms and decrease the number of subsequent surgeries are being investigated. Postoperative COC administration after conservative surgery for endometriosis has been shown to reduce the frequency and intensity of dysmenorrhea, 106 and GnRH agonist treatment has been shown to lengthen the period of pain relief. 107 Unfortunately, discontinuation of medical therapy results in the return of symptoms.
For women who no longer desire fertility and have debilitating pelvic pain, hysterectomy, bilateral salpingo-oophorectomy, and resection of endometriotic lesions are a treatment option when other medical and surgical treatments have failed. In premenopausal women, hormone therapy can be started with minimal risk of inducing growth of residual disease and return of preoperative symptoms. 108 In women with extensive endometriosis, it is advisable to have an interval of no hormone therapy, or progesterone-only therapy, in order to suppress residual endometriosis after definitive surgery has been performed.
Conclusions
Endometriosis is a complex and enigmatic disorder with medical and surgical management options customized to address the patient's symptoms and individual goals. As presented in this article, increasingly more evidence-based data is being published comparing surgical treatments and their outcomes. Currently, first-line management of endometriosis-associated pain includes NSAIDs and COC. Hormonal administration can suppress endometriosis-associated pain, but often this persists despite medical treatment, and recurs when medical treatment ceases. When medical therapy is suboptimal for managing endometriosis-related pain symptoms, thorough excision of the deeply infiltrating lesions, endometriomas, and associated scar tissue can alleviate pain and improve fertility. Prospective studies report a significant decrease in pain, general health, and psychoemotional status at 6 months after surgical excision. 109 At 2–5 years after laparoscopic excision of endometriosis, women still reported significantly reduced pain and improved quality of life, but 36% of women required additional surgery. 110 Therefore, management of endometriosis and its associated symptoms is challenging and requires a multidisciplinary approach. Current research and therapeutic strategies aimed at preventing or halting the inflammatory sequelae of endometriosis will allow gynecologists to offer women more efficacious conservative treatments in the future.
Footnotes
Acknowledgments
We thank Susan Kearney for her editorial expertise.
Disclosure Statement
Drs. Dun and Dr. Wieser have no conflicts of interest. Dr. Nezhat is a consultant for Conceptus, Hologic, Lumenis, Intuitive Surgical, and Karl Storz; medical advisor for Plasma Surgical; and on the scientific advisory board for SurgiQuest.
This article was supported by Grants UO166439 and 1R21HD065115-01.