
Abstract
Abstract
Introduction
M
Damage control surgery (DCS)/damage control laparotomy (DCL) is defined as rapid termination of an operation after control of life-threatening bleeding and contamination, followed by correction of physiologic abnormalities and definitive treatment. DCS/DC avoids extensive procedures on patients with unstable conditions, stabilizes the effects of potentially fatal problems during the initial operation, and applies staged surgery after successful initial resuscitation. Thus, surgical interventions are abbreviated before the development of irreversible physiologic endpoints: hypothermia; coagulopathy; and acidosis. Each of these life-threatening abnormalities exacerbates the others, rapidly resulting in death unless hemorrhaging is stopped, and the abnormalities revert to their formerly normal status. 5
During the first stage of damage control, hemorrhaging is stopped, and contamination is controlled using the simplest and most-rapid means available. Temporary wound closure methods are used. The second stage is characterized by correction of physiologic abnormalities in the intensive care unit (ICU). Patients are warmed and resuscitated, and coagulation defects are corrected. In the final phase of damage control, definitive operative management is completed in a patient in a stable condition. 5
Surgical options used to treat PPH include repair of genital-tract trauma, evacuation of retained products of conception, uterine-balloon tamponade, exploratory laparotomy and uterine compression sutures, systematic pelvic devascularization, uterine artery embolization, and subtotal or total abdominal hysterectomy. It is of paramount importance that obstetricians and surgeons be familiar with the various surgical measures available that could be used to arrest hemorrhaging, the appropriateness of a chosen surgical intervention to the specific clinical situation, and the timing of instituting the intervention.3,4,6
A case of a patient with massive PPH that was treated using the damage-control approach by surgical gauze–packing of the pelvis and laparostomy after failure of conventional treatment, is presented in this article.
Case
A 36-year-old woman, gravida 4 para 3, presented in labor to the maternity ward at Clinicas Hospital at the Federal University of Minas Gerais, Santa Efigênia, Belo Horizonte, Minas Gerais, Brazil. She was in the 38th week of pregnancy with a breech presentation. Her obstetrical history revealed three pregnancies that were ended by caesarean delivery (CD). She presented with chronic hypertension and was taking methyldopa (500 mg b.i.d.). Her blood pressure was 190/120 mm Hg. A vaginal examination revealed no effacement or dilatation, and no bleeding or amniotic-fluid leakage. Laboratory studies showed the following results: serum creatinine level of 0.6 mg/dL; serum aspartate aminotransaminase (AST) level of 40 U/L; uric acid level of 6 mg/dL; hematocrit 35.2%; and platelet count 173×103/mm3. A catheterized urine sample showed no proteinuria. CD with the patient under spinal anesthesia was performed <60 minutes after admission. The placenta was attached strongly to the uterine wall. Manual removal with curettage was performed in an attempt to extract the placenta fully. Once the uterine incision was closed, no source of bleeding was found, and active bleeding had subsided. Her blood loss was estimated to be ∼800 mL, and she was transferred to the postanesthesia recovery unit. One hour later, uterine atony was identified, with blood mildly oozing per vaginum. Her oxytocin infusion was, therefore, increased to 20 U. Her vital signs were unstable, and laparotomy was immediately performed with her under general anesthesia. At laparotomy, uterine atonia was diagnosed, and a subtotal hysterectomy with bilateral internal iliac artery ligation was performed. At the end of surgery, the patient's vital signs were stable and her laboratory results were within the normal reference ranges. She was transferred to the ICU, and 12 hours later, presented with major hemorrhagic shock (hemoglobin 2.0 g/dL), acute renal failure (rise in creatinine level from 0.6 to 1.6 mg/dL), metabolic acidosis (pH 6.93, serum bicarbonate 5 Mmol/L, base excess −24 Mmol/L, and a lactate level of 132 mg/dL), hypothermia (34.2°C at the nasopharynx), diffuse coagulopathy (a platelet count of 24×103/mm3, partial thromboplastin time showing no coagulation, and a fibrinogen level 92 mg/dL), and hyperkalemia (7.4 mEq/L). A new laparotomy was performed, which revealed massive hemoperitoneum (3 L) as well as active bleeding from the hysterectomy site. The patient's pelvis was packed firmly with three large laparotomy packs followed by a temporary abdominal closure with a Bogotá bag. The total operative time was 50 minutes (Fig. 1). Massive volemic resuscitation—with a total infusion of 10 U of packed red blood cells, 32 bags of platelets, 15 U of fresh frozen plasma, 17 L of crystalloids, and 2 L of hydroxyethyl starch within 24 hours—was performed. The patient was rewarmed to 37°C in 4 hours by maintaining room temperature at 28°C, infusion of warm fluids, and the use of a forced air warming device. A scheduled reoperative procedure was performed 48 hours later after improvement in this patient's temperature, base excess, and coagulation profile. As there was no active bleeding, the packs were removed. Her abdomen was closed with closed-suction drainage.
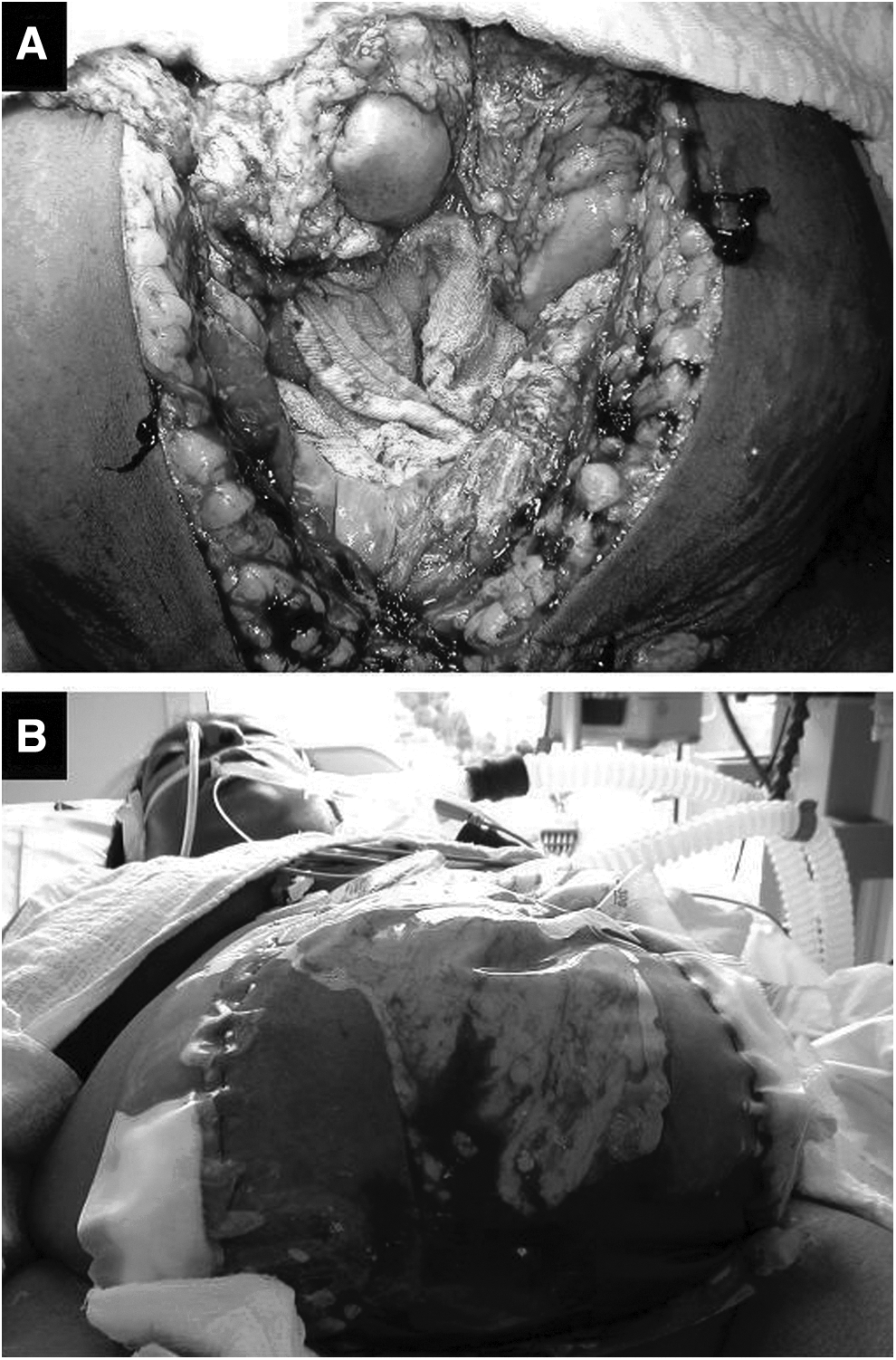
Damage control in the management of a patient with massive postpartum hemorrhage.
Results
This patient stayed in the ICU for 3 days. Her vital signs and results of laboratory studies improved, and she had no evidence of further intraabdominal bleeding. She was discharged to go home on postoperative day 10 with her healthy newborn. Both the mother and newborn remained well at follow-up.
Discussion
Massive PPH accounts for almost half of the postpartum maternal mortalities in developing countries and is the major cause of maternal death worldwide.1,2 Prevention, early recognition, and prompt intervention are the keys to minimizing complications. However, even with major advances in prevention, ∼3% of all women will have severe PPH.2,3 The general condition of a patient, her hemodynamic stability, the amount and rate of bleeding, the effectiveness of conservative measures, the likely cause of PPH, and the skill and experience of the obstetrician/surgeon, as well as the availability of resources, should be considered in the decision-making process.2–4
The basic principles of PPH management involve relieving the causative factors (especially surgically correctable injuries) and prompt replacement of intravascular volume, blood, and coagulation factors as needed. Surgical therapies may be divided into four groups: (1) those that decrease blood supply to the uterus; (2) those that remove the uterus; (3) those aimed at causing uterine contraction or compression; and (4) those that tamponade the uterine cavity. Surgical management for intractable PPH includes uterine artery embolization, laparotomy with ligation of the uterine vessels or internal iliac arteries, and hysterectomy.2–4
Emergency hysterectomy has been widely considered as a lifesaving measure to manage intractable uterine hemorrhage. Indications include abnormal placentation (previa, accreta), atony, trauma, rupture, and sepsis. The disadvantage of peripartum hysterectomy is the loss of fertility in women who wish to continue childbearing.3,4 The American College of Obstetricians and Gynecologists recommends, however, that if hysterectomy is performed for uterine atony, there should be documentation of first attempting other therapies.2,4
A variety of techniques have been used to tamponade the uterine cavity. Such techniques include uterine packing, the umbrella pack, the Sengstaken–Blakemore balloon, and a variety of other adapted balloons and packs. Some obstetricians have even used a large, inflated Foley catheter. Uterine packing has been shown to be a safe and effective technique in the control of intractable hemorrhage in CD. It is a reasonable alternative to further surgical intervention in patients with intractable obstetric hemorrhage, especially in developing countries, or in patients with intractable obstetric hemorrhage who wish to preserve fertility. Disadvantages, however, include risk of infection, unrecognized bleeding with blood soaking the packing material, and the possible need for another surgical procedure to remove the material.5,6
Unfortunately, some patients will have persistent bleeding even after hysterectomy. Diffuse posthysterectomy bleeding from peritoneal surfaces associated with consumptive coagulopathy may be controlled by abdominal packing.5,6 However, once metabolic failure has become established, it is extremely difficult to control hemorrhage and correct the physiologic derangements.
The term “damage control” refers in this context to an approach to patients with life-threatening injuries and consists of rapid surgical techniques to control hemorrhaging (intraabdominal packing) and temporary abdominal closure. 7 DCL or DCS improves outcomes when used in patients with severe hemorrhaging. Correction of coagulopathy with close ratio resuscitation, while limiting crystalloid, is a new methodology referred to as damage control resuscitation (DCR). 8 The patient is transferred to the ICU for restoration of temperature, coagulation, perfusion, and ventilation. Removal of abdominal packs, definitive surgery, and abdominal closure are performed after improvement in the patient's physiologic state. The combination of hypothermia, coagulopathy, and acidosis is a syndrome that accelerates its effects in a cycle that is rapidly fatal unless it is interrupted. 9 Patients are more likely to die from this triad than from failure to complete operative repairs. 10 The criteria in decision making for damage control are hypotension (systolic blood pressure [BP] <90 mm Hg), hypothermia (<34.8°C), coagulopathy (partial thromboplastin time >60 seconds) and acidosis (pH <7.2 base excess <−8).10,11 This technique has been shown to increase overall survival and is likely to modify the management of the critically injured patient. Simplicity is the key in damage control, in which sometimes less is more. It is not currently known whether DCL/DCS is superior to immediate surgery for patients with major abdominal trauma. 7
Conclusions
PPH requires early recognition of its cause; immediate control of the bleeding source by medical, mechanical, invasive nonsurgical, and surgical procedures; rapid stabilization of the mother's condition; and a multidisciplinary approach. Second-line treatment of PPH remains challenging, because there is a lack of univocal recommendations from current guidelines and sufficient data from randomized controlled trials. 12 The damage-control concept, however, may offer an option to optimize management of patients with life-threatening PPH.
Footnotes
Disclosure Statement
No competing financial interests exist.