
Abstract
Abstract
Introduction
In recent years, laparoendoscopic single-site (LESS) surgery has been introduced into clinical practice as a minimally visible scar surgery.5,6 Through an incision eventually concealed within the umbilicus, LESS surgery can now be applied to a wide range of surgical procedures. However, there are potential difficulties in extracting bulky solid tumors without elongation of the umbilical incision, and the abdominal wound required for tissue retrieval could continue to be a major source of potential surgical morbidity.
Natural orifice specimen extraction (NOSE) has been proposed as a procedure to retrieve the excised tissue through a natural orifice such as the vagina or anus without the need for either further elongation or addition of abdominal wall incision. 7 However, application of the NOSE technique in gynecologic LESS surgery has never been described. The successful application of transvaginal NOSE with a wound retractor attached through posterior colpotomy for management of large ovarian fibroma with extensive calcification in LESS surgery is reported here.
Case
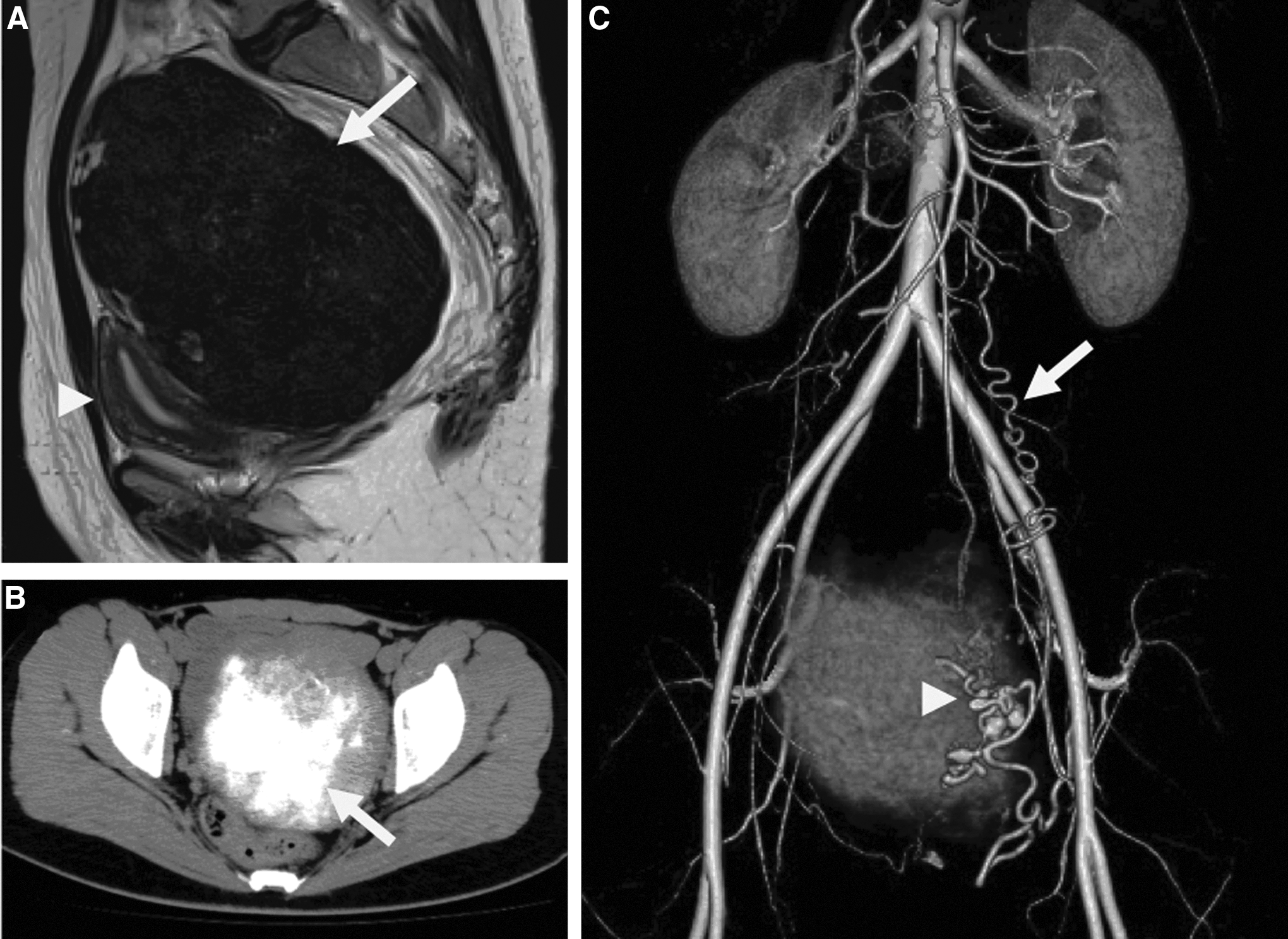
A 24-year-old nulligravida was referred for a pelvic mass found at a regular checkup, with suspicion of large subserosal myoma. On magnetic resonance imaging (MRI), a well-demarcated tumor measuring 12.7×10.6×10.9 cm (Fig. 1A, arrow) was noted in the left posterior side of the uterus (Fig. 1A, arrowhead). The pelvic tumor showed heterogeneous signal intensity that was mostly hypointense compared with uterine myometrium on a T2-weighted image. Computerized tomography (CT) showed extensive calcification in the central portion of the tumor (Fig. 1B, arrow). The arterial phase of three-dimensional CT angiography 8 showed an aneurysm-like dilatation of the ascending branch of the left uterine artery (Fig. 1C, arrowhead) that fed the calcified tumor. Anastomosis of the ascending branch with the left ovarian artery (Fig. 1C, arrow) was also noted.
Because of suspicion of left solid adnexal tumor based on CT angiographic findings, gasless LESS surgery6,9 was performed. A 2.5 cm midline umbilical skin incision was made vertically and carried down into the peritoneum. An Alexis O wound retractor (small size, Applied Medical, Rancho Santa Margarita, CA) with a rigid retraction ring was placed in position through an umbilical incision with the bottom green ring inside the abdomen. The surgical view was secured by the abdominal wall lift method with an intra-abdominal fan retractor system (Mizuho Co., Tokyo, Japan). 9 Under laparoscopic observation, a left solid ovarian tumor with prominent vascularization (Fig. 2A, arrow) was identified. As normal ovarian parenchyma was difficult to identify under laparoscopic vision, a left salpingo-oophorectomy was performed with Ligasure Atlas (Tyco Healthcare, Tokyo, Japan) (Fig. 2B).

It seemed extremely difficult to remove excised bulky solid tissue from the body through the umbilical wound without significant extension. Therefore, posterior colpotomy was performed for vaginal extraction. To obtain maximum expansion of the vaginal canal for tissue retrieval in addition to wound protection, an Alexis O wound retractor was transvaginally placed through the posterior colpotomy in position with the rigid green ring at the cul-de-sac (Fig. 2C and D).
Through the transvaginally attached wound retractor, the solid ovarian tumor was grasped with Museux-type grasping Tenaculum forceps and was morcellated into small pieces with either a cold scalpel or scissors (Fig. 2C) under laparoscopic monitoring. The outer part of the tumor composed of a rather soft component (Fig. 2D, arrow) could be morcellated using a cold knife; however, the central calcified portion (Fig. 2D, arrowhead) was extremely hard to cut with a cold knife. Therefore, the soft outer portion was peeled off first using a cold scalpel. Then, the calcified portion was put into an ENDOPOUCH RETRIEVER® (Ethicon Japan, Tokyo, Japan) to prevent dispersal of small calcified pieces in the abdominal cavity and was fragmented using a scissors. After the surgical procedures were completed, the abdominal cavity was extensively washed with saline.
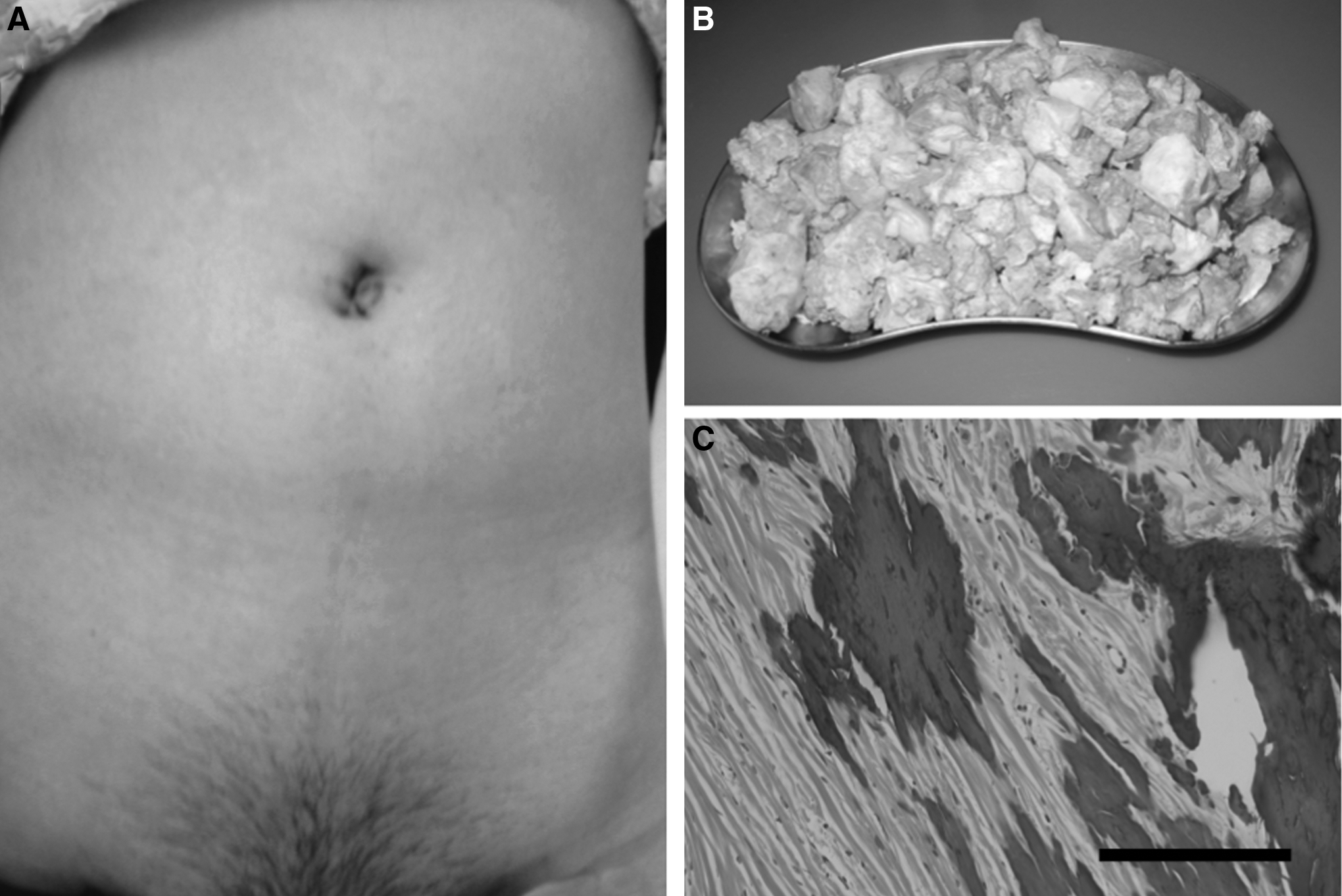
After the surgical procedures were completed, the abdominal cavity was extensively washed with saline and the vaginal wound retractor was removed. The posterior colpotomy incision was closed with 1-0 Vicryl (Ethicon Japan, Tokyo, Japan). Then, hemostasis and adjacent organ injury were finally inspected. After removal of the umbilical wound retractor, the umbilical fascia was closed with 1-0 Vicryl and the umbilical subcutaneous tissue was approximated with 3-0 Vicryl (Fig. 3A).
Results
The excised tissue weight was 854 g (Fig. 3B) and blood loss was 80 mL. Surgical duration was 172 minutes, including 110 minutes required for tissue retrieval through the vagina. The postoperative course was uneventful. Pathologic diagnosis was ovarian fibroma with extensive calcification (Fig. 3C).
Discussion
Ovarian fibroma is a benign solid neoplasm that arises from the connective tissue stroma of the ovary. 1 In addition to initial ultrasonographic evaluation, MRI is the established imaging modality to evaluate ovarian pathology, especially when differential diagnosis from pedunculated subserosal myoma is required. 2 However, as various degrees of secondary change can alter the imaging pattern in both ovarian fibroma and uterine myoma,2,4 there are still potential difficulties in differentiating ovarian fibroma from subserosal myoma before surgery.
The diagnostic value of three-dimensional CT angiography is not well established in gynecologic disorders, and its clinical application in gynecologic diagnostic imaging is still limited. 8 In the present case, three-dimensional CT angiography clearly showed characteristic aneurysm-like dilation of the feeding left uterine artery that anastomosed with the left ovarian artery, indicating the ovarian origin of the present tumor rather than subserosal myoma.
With the recent developments of surgical equipment and techniques, laparoscopic surgery is progressing toward reduced port surgery 10 that is represented by natural orifice translumental endoscopic surgery 11 or LESS surgery5,6,9 in order to reduce the incisional morbidity and improve the cosmetic outcomes further. However, a major obstacle in no-scar or minimum-visible-scar surgery is the extraction of large, bulky, or rigid specimens.6,7,12
NOSE is a newly emerged concept to remove tissue without addition or elongation of the surgical wound in the abdominal wall. 7 This potentially decreases the incidence of surgical wound complications and improves the cosmetic outcomes. The vagina has been established as a specimen extraction route in the NOSE technique because of its improved healing, elasticity, and cosmetic superiority. 7 The Alexis wound retractor was successfully used to extract large myomatous uteri through the vagina in laparoscopic hysterectomy. 13 As indicated, a wound retractor can help to prevent vaginal lacerations, tears, and bruising caused by a retractor that has sharp edges. 13 In the present case, use of a wound retractor was initially aimed to protect the vaginal canal during tissue extraction. Thereafter, it became evident that a wound retractor alone can maintain maximal expansion of the vaginal canal because of its superior elasticity and flexibility, thus facilitating the extraction procedure. Furthermore, it can prevent excessive pressure being placed on the vagina during the extraction of extensively calcified ovarian fibroma.
Conclusions
A large ovarian fibroma with extensive calcification was successfully excised by LESS surgery with transvaginal NOSE technique using a wound retractor after diagnostic imaging. Transvaginal NOSE could be potentially useful to extract bulky specimens in gynecologic LESS surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.