
Abstract
Abstract
Introduction
C
Case
The case of a 57-year-old gravida 4, para 3, woman who, according to her statement, had incidentally found that she had a pelvic mass 15 days prior to her visit to the outpatient department (OPD), is presented. There was no postmenopausal bleeding, abdominal pain, or fullness. She reported recently increased urinary frequency. She referred to a weight loss (∼5 kg) during the previous 2–3 months. Past gynecologic, surgical, and medical histories were unremarkable. On examination, abdominal distension and right lower abdomen tenderness were found. A transvaginal ultrasound (TVS) was performed, and revealed a complex pelvic mass, with solid and cystic components, measuring ∼15×11 cm, and probably arising from the right ovary (Fig. 1). A computed tomography (CT) of the abdomen and the pelvis showed a complex cystic mass with peripheral enhancement and roughly the same size as that reported on the TVS (Fig. 2). All laboratory data, including serum tumor markers, were within normal limits. Laparotomy was performed. Intraoperative findings revealed a large cystic tumor of the right ovary, with a solid component, and 600 mL of bloody fluid was collected. The uterus, the left ovary, and bilateral Fallopian tubes were of normal appearance. Bilateral salpingo-oophorectomy (BSO) was performed. The fresh specimen was sent for frozen section evaluation. Gross examination showed a tumor with a solid component measuring 11.4×8.2×4.7 cm (Fig. 3). This solid component was yellow and firm. The external surface of the tumor was smooth, with hemorrhage.

Transvaginal ultrasound showing a complex cystic mass with an evident solid component.
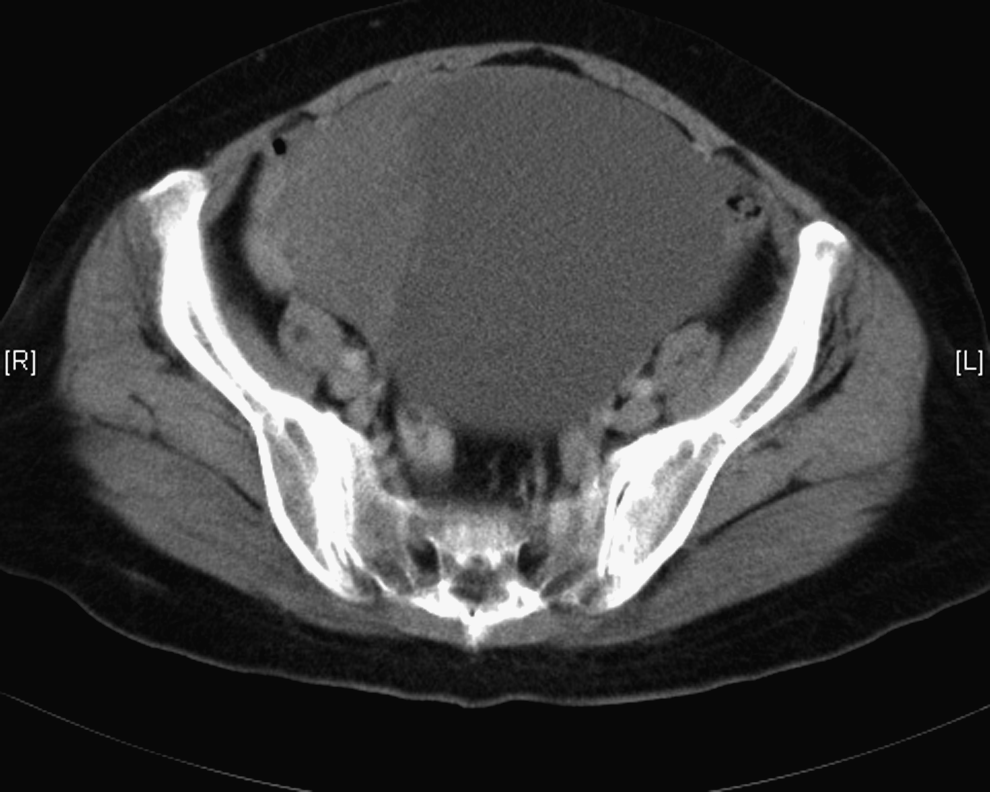
Computed tomography revealing a peripheral enhancement of the complex cystic mass.

Gross examination demonstrating the solid component of the tumor, with a yellow and smooth surface.
Results
All of these findings suggested a benign ovarian tumor, probably an SST or massive stromal edema. Microscopically, the tumor consisted of alternating hypocellular/edematous areas and hypercellular areas, prominent vessels and areas of sclerosis (Fig. 4). Based on the histologic features described, the diagnosis of SST was made. The patient recovered well after surgical intervention.
Histologically, the tumor consisted of hypercellular and hypocellular areas (hematoxylin and eosin [H&E] stain, 100×).
Discussion
SSTs are a distinct subtype of ovarian stromal tumor. Roughly 120 cases have been reported in the English literature. 3 They account for <5% of all sex cord stromal tumors. 5 Usually they are found in young women, within the second and third decades of life.2–5 Other types of stromal tumors are generally found in the fifth and sixth decades of life. However, there are reports of SST in postmenopausal women. 5
Symptoms can range from premature menarche, menstrual irregularities, abdominal discomfort, pain, or mass, and, rarely, ascites.
There is also a degree of uncertainty about the hormonal activity of SSTs. Data in the literature are conflicting, because some investigators described steroid function in these tumors.6–8 A few of these reports included several patients with irregular menstrual cycles who, after tumor excision, regained regular menses. However, the hormonal activity of an SST was clearly demonstrated in pregnant women. The study, by Quinn et al., reported an SST in a patient with an ectopic pregnancy, with preoperative elevated androgen levels and an elevated androstenedione-to-testosterone ratio, which are unusual findings during pregnancy. 8 Another report, by Lam and Geittmann, demonstrated that the cells of an SST were enzymatically active for estradiol 17-β-dehydrogenase, glucose-6-phosphate dehydrogenase, and isocitric dehydrogenase, but not for 3β-ol-hydroxysteroid dehydrogenase and testosterone 17-β-dehydrogenase. 9 According to these findings, the authors concluded that the SST cells were able to synthesize dehydroepiandrosterone via five different pathways.
Histologically, the main features of SST are the presence of pseudolobulation of cellular areas, separated by edematous connective tissue, increased vascularity, and prominent areas of collagenous sclerosis. 2 Immunohistochemistry may be of help in clarifying the diagnosis, because SST is usually positive for muscle-specific actin, and immunoreactivity is intense in hypercellular areas. Vimentin is diffusely positive, and desmin may also be focally positive in SST. 3 One other study, focused on immunohistochemical analysis of SST, paid special attention to its vasculature. 9 The authors demonstrated expression of vascular permeability factor (VPF) and vascular endothelial growth factor (VEGF) in the luteinized theca-like cells and the receptor capillaries, and even in medium-sized blood vessels.
To date, all reported cases of SST are clinically benign, and surgical removal of the tumor is curative. Local or distant tumor relapse has not been described. There is one report of an SST with elevated CA-125; however, there are no specific markers for this kind of tumor.
Imaging modalities can demonstrate both specific and nonspecific features. The ultrasound appearance of SST is that of a complex mass, with both cystic and solid areas. Color Doppler ultrasonography may reveal prominent vascularity in the periphery and in central intercystic spaces. 5 CT can also be useful, but magnetic resonance imaging (MRI) may prove to be far more effective. Typical MRI findings of an STT include pseudolobulation, demonstrated by low-intensity nodules, as opposed to the high-intensity stroma on T2-weighted images. 4 This is explained by the fact that the densely packed cellular areas are associated with multiple foci with sclerosis, which explains the low-intensity images on T2-weighted images. On the other hand, high-intensity areas on T2-weighted images have a direct correlation with the edematous tissue of hypocellular areas. However, the value of MRI in the distinction among SST, other types of stromal tumors, and metastatic ovarian tumors remains to be established.
Conclusions
Differential diagnosis for SST includes subserosal leiomyomas, epithelial ovarian cancers, and sex cord stromal tumors. Typically, parauterine leiomyomas show lower or similar signal intensity compared with normal myometrium on T1-weighted images. On T2-weighted images, myomas usually show lower intensity. Thecomas and fibrothecomas usually show extremely low signal intensity on T2-weighted images. Granulosa cell tumors typically have hormonal activity, and are frequently hemorrhagic. Malignant tumors of the ovary exhibit features such as invasive growth, which distinguish them from benign neoplasms.
This reported case was somewhat unusual, because the patient was a postmenopausal woman, and also because of the large tumor size.
Footnotes
Disclosure Statement
No competing financial interests exist.