
Abstract
Abstract
Introduction
Proper diagnosis and treatment can be elusive if based on clinical symptoms and the character of the vaginal discharge alone. Inadequate or improper treatment leads to a lack of symptomatic relief and increased costs to the patient. 2 In dermatologic mycology, direct microscopic examination and culture serve as the main diagnostic procedure tools. 3 Microscopic examination of a wet KOH preparation is usually satisfactory for the detection of non-species-specific fungal infection. It is possible to identify the specific infecting organisms based on the morphologic characteristics of the fungal elements; however, examination of the KOH wet mount requires skill and experience. In order to help unskilled personnel to recognize fungal elements by microscopic examination, a number of differential strains have been described. Great strides have been made to improve the sensitivity and specificity of direct microscopy and chemical cell wall analysis for the detection of fungal species.4,5
The purpose of this study was to determine the diagnostic concordance between standard light microscopic images obtained during the wet mount examination and fungal culture results obtained from the same patients with a history of recurrent fungal vaginal colonization.
Whether these morphologic features are useful for differentiating Candida albicans from other yeast species has not previously been systematically evaluated.
Methods
This retrospective cohort study took place in the outpatient university-affiliated faculty private office from January 2006 to December 2010. Only patients with three or more symptomatic recurrences documented by positive fungal culture were included in the study.
According to the study protocol, if patients presented with recurrent vulvovaginal symptoms (vulvar or vaginal pruritus, redness, burning, “white cheese” discharge), then two vaginal swab specimens were simultaneously obtained. One swab was placed in sterile physiological saline solution and prepared for immediate microscopic examination (wet mount) and KOH (potassium hydroxide) examination. The second specimen was placed in the transportation media (sterile red tube cotton swab) to Compunet Laboratories where it was subsequently cultured on Sabouraud dextrose and brain–heart infusion agar media and incubated at 30°C and 37°C for 30 days.
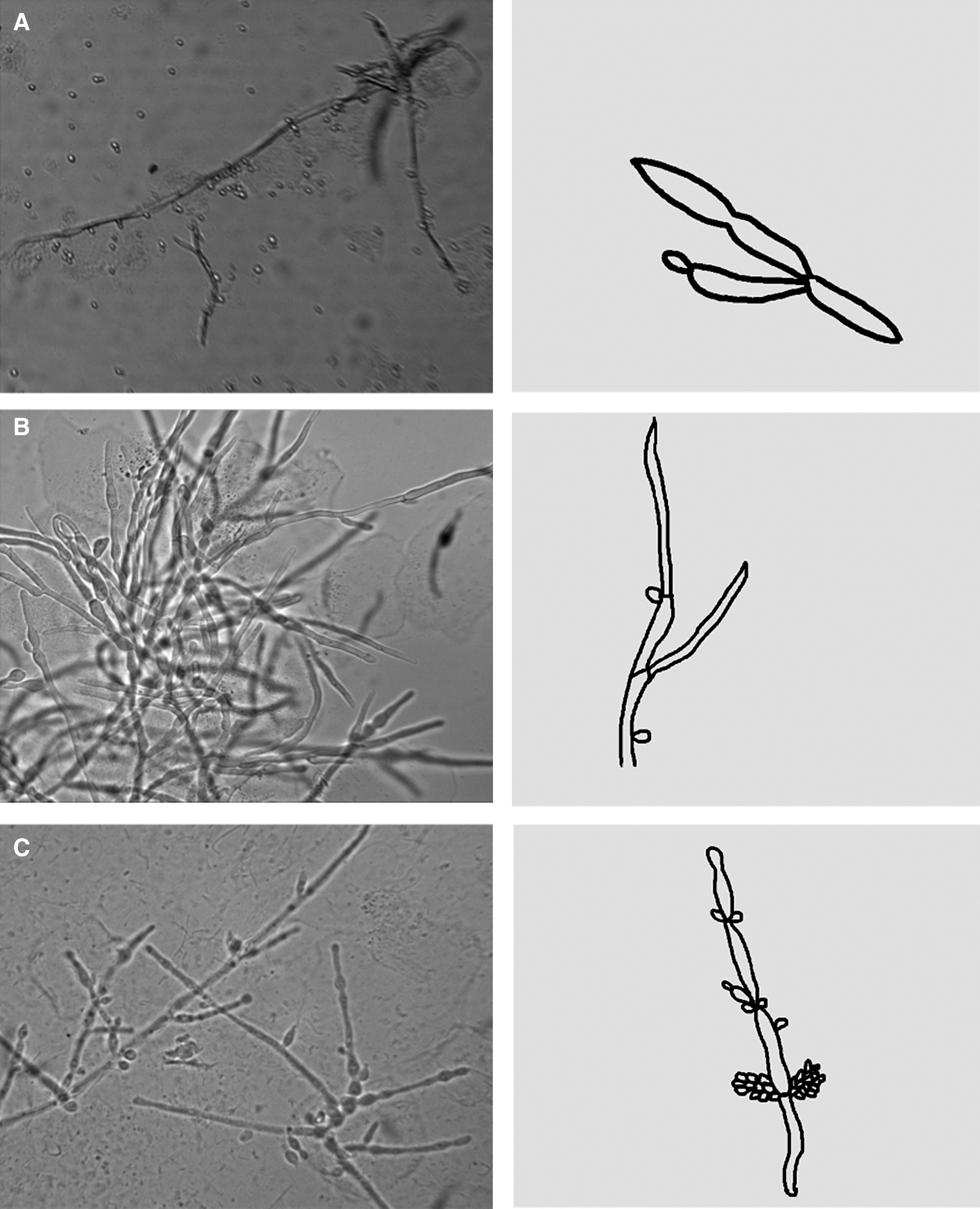
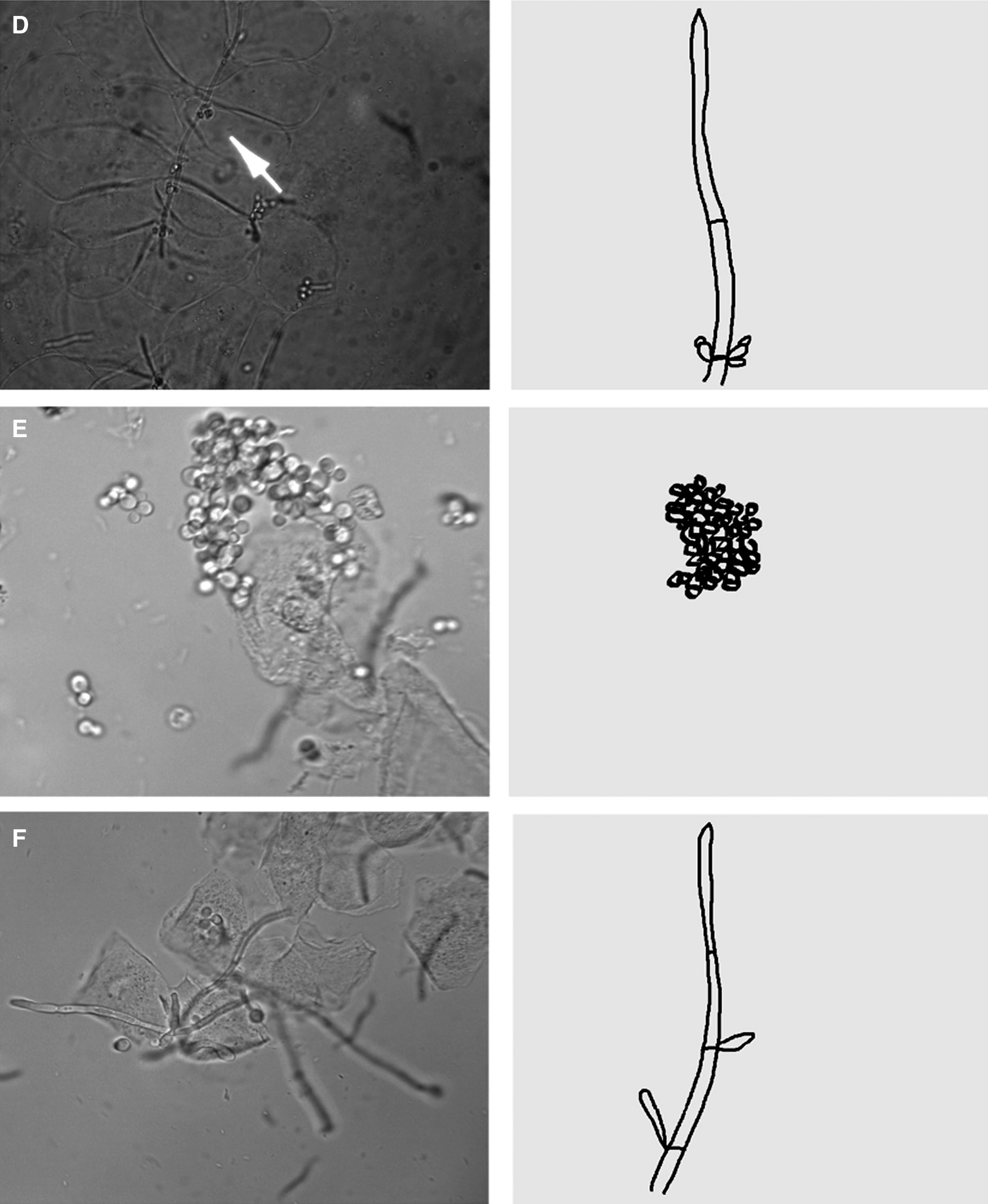
At least three images were obtained of each microscopic slide; the slides were made by an experienced clinician. An initial fungal infection was diagnosed, and microscopic images were taken. The images were then reviewed by a trained microbiologist and a trained pathologist, both blinded to the culture results. Any discordance regarding an image interpretation was resolved by mutual agreement.
Diagnoses rendered by the fungal culture were compared with the original light microscopic fungal diagnosis based on morphologic visualization of clusters of pseudohyphae at the KOH wet mount examination.
Samples from pregnant patients, women who had been treated with antibiotics or antifungals within the previous 4 weeks, women with a history of immune compromise, women currently taking corticosteroids, and women who had a history of vaginal douching, were excluded.
The seven most common positive fungal culture results obtained from 2006 to 2010 were recorded. The images were then matched with culture results.
The study was Institutional review board–approved. Statistical analysis was performed using Graph Pad. A p-value<0.05 was deemed to be significant.
Results
One hundred and sixty-seven patients were screened for cultures, microscopic images and correlating results. Ten patients (6%) did not have their respective microscopic pictures saved or were not optimal for morphologic identification, and 4 patients (2.4%) did not have documentation of their initial prescribed therapy. Therefore, 153 (91.6%) samples were included in the study.
The identification of fungi species, from wet mount microscopy samples, did not correlate with the species culture 75% of the time and was positively correlated only 25% of the time (p=1).
The seven most common fungal cultures that were reported included C. albicans 75%, C. glabrata 14%, C. krusei 5%, C. parapsilosis 3%, C. tropicalis 2%, and C. famata 1%, and C. lusitaneae 1%.
Discussion
Vaginal discharge is one of the most common women's healthcare problems in the United States. 6 Infectious vaginitis is responsible for between 5,000,000 and 10,000,000 clinic visits annually, with related healthcare costs of >$500,000,000 each year. 7 The three leading agents that cause 90% of infectious vaginitis are bacterial vaginosis, fungal infections, and parasitic infections.
Culture media are widely applied for isolation and identification of candida species from clinical specimens. In dermatologic mycology, the predictive diagnostic value of a diagnostic test has to be delineated for each disease state. As an example, based on the current study results, direct microscopy is a useful diagnostic procedure for the general presence of candida infection, but is only correct 25% of the time in determining the candida species. This study is also important because of the high recurrence observed in patients diagnosed with non-albicans species, as described by Ventolini et al. 8
Sobel reports that three quarters of all adult women experience at least one episode of candidiasis during their lifetimes, with ∼5% having recurrent infections. 9
Siapco et al. reported a similar study, although they used cervical smears and cervical scrapings cultured on Sabouraud agar from 31 women suspected of having candida genital infections, who were examined in a study of the cytomorphology of fungal infection in cervical smears. These researchers observed that although the sensitivity of the cervical smear in detecting fungus in culture-positive patients was only 80%, the cervical smear can still be a useful means of rapid identification of C. albicans when blastospores and pseudomycelium are present. In addition, the researchers concluded that the presence of budding or nonbudding yeast without pseudohyphae should strongly suggest a Torulopsis glabrata infection. 10
In another study about fungal morphology, Odds et al. reported that the microscopic morphology of their isolates was scrutinized by four individuals experienced in yeast identification, and three inexperienced persons, all of whom were blinded as to the putative identification of the yeasts. For 49 (70%) of the 70 isolates, the seven observers recorded comparable scores for morphology, but 5 (7%) of the isolates showed extreme variation in recorded morphologies, from true hyphae formed to no pseudohyphae formed. Isolates of C. parapsilosis and T. glabrata consistently did and did not form pseudohyphae, respectively. Their results showed that pseudohypha formation is not a reliable characteristic for identification of yeasts at the genus level, and they suggested that the merger of Torulopsis spp. into the genus Candida should be finally accepted, as it is nowadays. 11
In 1997, Bale et al. proposed an evaluation of growth characteristics on blood agar and eosin methylene blue agar for the identification of C. (T.) glabrata. 12
In much older yeast taxonomies, different styles and appearances of pseudohyphae were used to distinguish yeast taxa; however, these characteristics were later abandoned, largely because of their variability.4,5
The presence of pseudohyphae clusters by gram stain of blood cultures is nevertheless useful for distinguishing C. albicans from non-albicans yeast according to Harrington et al. They concluded that additional studies are necessary to determine the clinical impact of these findings and their validity with other blood culture systems. 3
Conclusions
Based on these findings, taking culture specimens from patients with symptomatic recurrent vaginal colonization who are positively identified as colonized by fungi at a wet mount microscopy, should be considered.
Footnotes
Disclosure Statement
The authors disclose that they do not have any competing financial interests.