
Abstract
Abstract
Introduction
Case
A 51-year-old woman presented with bleeding per vaginum of 15 days' duration. She also complained of nausea and vomiting of 1 months' duration. She had been in a natural menopause for 15 months. Her obstetric history showed three normal vaginal deliveries, and her last pregnancy was 20 years earlier. She had no history of gestational trophoblastic disease. Examination revealed an enlarged uterus of 16 weeks' size. Ultrasound of her pelvis revealed a vesicular sonographic pattern inside the uterus and no adnexal pathology (Fig. 1). Because of this finding, a pregnancy test was obtained, resulting in a quantitative serum β-human chorionic gonadotropin (hCG) of 244000 milli-international units (mIU)/mL. Other systemic examination revealed no other abnormalities. A presumptive diagnosis of hydatidiform mole was made. Preoperative chest radiograph, complete blood count, thyroid function tests, and blood chemistries were within normal limits. Computed tomography (CT) scan of the abdomen and pelvis was obtained in view of possible choriocarcinoma in this postmenopausal patient. However, it was remarkable only for an enlarged uterus containing heterogeneous material. Exploratory laparotomy revealed an enlarged uterus but no other abnormal findings. Total abdominal hysterectomy and bilateral oophorectomy were completed without complications.

Ultrasound of the pelvis showing characteristic vesicular sonographic pattern inside the uterus.
Results
The total abdominal hysterectomy specimen consisted of a 15 cm×11 cm×8 cm uterus with bilateral Fallopian tubes and ovaries. Macroscopic examination revealed an enlarged endometrial cavity containing blood clots, and multiple grapelike transparent vesicles measuring up to 1.5 cm in diameter (Fig. 2). Microscopic examination of the endometrial tissue specimens revealed generalized hydropic villi and proliferation of trophoblastic cells. The histomorphologic findings were suggestive of benign noninvasive complete mole. Postoperatively, quantitative serum β-hCG levels were followed weekly until they reached the normal range after 12 weeks. Levels were checked monthly for 1 year thereafter and remained normal. On follow-up, the patient remains without evidence of post-molar gestational trophoblastic tumor (GTT).
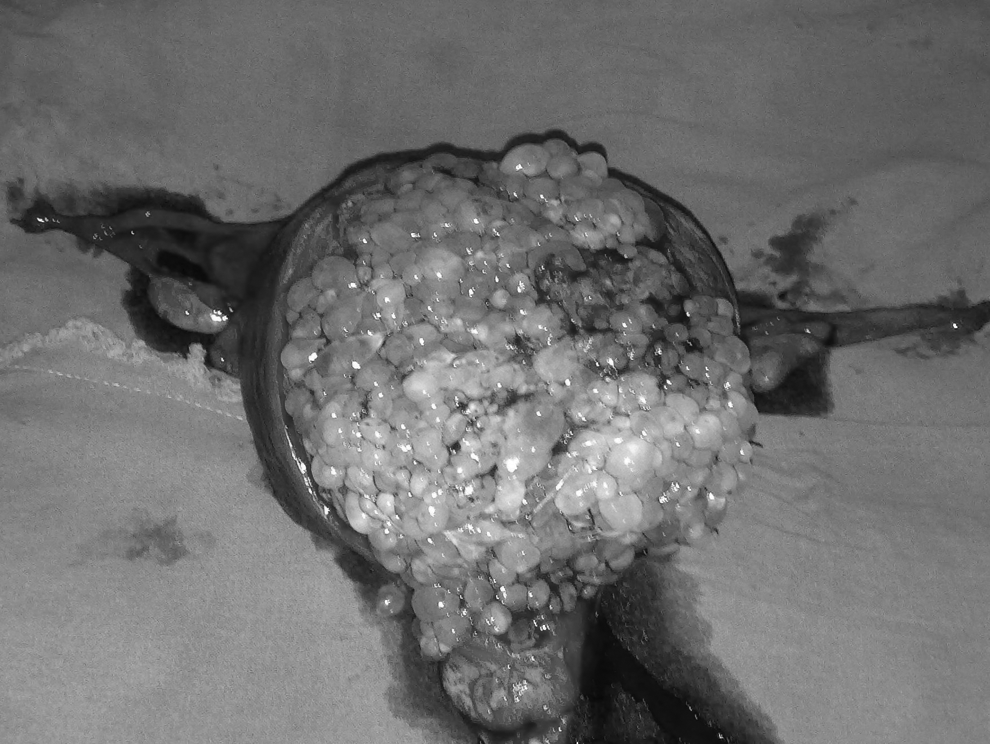
Photograph showing uterus with an enlarged endometrial cavity containing multiple grapelike transparent vesicles and bilateral Fallopian tubes and ovaries.
Discussion
Hydatidiform mole is rare in women of postmenopausal age. In contrast to moles occurring during the reproductive years, postmenopausal GTNs seem to evolve independently of gestation. Spontaneous ovulation followed by defective fertilization may be the initial event in the development of GTN. A latent GTN that remains dormant for long periods and becomes clinically evident in the postmenopausal period is thought to occur through another mechanism. 4 Ultrasonography has been accepted as a method for the diagnosis of complete molar pregnancy, because the marked swelling of the chorionic villi produces a characteristic vesicular sonographic pattern. 5 In younger women, this is usually accomplished by suction curettage with an associated risk of post-molar GTT in ∼20%. However in women >35 years of age, the risk of post-molar GTT after suction curettage appears to be increased and is reported to be as high as 56% in women >50 years of age. In these women who may have completed their childbearing, evacuation via hysterectomy offers the advantage of simultaneous treatment and sterilization and appears to decrease the risk of postmolar GTT. 6 However, there remains an 8%–20% risk of postmolar GTT in the elderly gravida after hysterectomy,6,7 and, therefore, close follow-up with serum β-hCG is indicated.
Conclusions
In perimenopausal and postmenopausal patients >50 years of age, a proper diagnosis of hydatidiform mole can be difficult, because of its low occurrence and presentation in unusual situations. Although rare, the diagnosis of hydatidiform mole should be kept in mind when evaluating patients with postmenopausal bleeding.
Footnotes
Disclosure Statement
No competing financial interests exist.