
Abstract
Abstract
Introduction
Case
A 27-year-old African American woman presented to the emergency department 5 days after an uncomplicated cesarean delivery, reporting sharp, intermittent right-sided flank pain. She also had decreased appetite, nausea, and subjective fevers, but no dysuria or abnormal vaginal discharge. Physical examination in the emergency department revealed normal bowel sounds and tenderness to palpation in the right lower quadrant and right costovertebral angle. No abdominal guarding or rebound tenderness was noted. Her cesarean incision was clean, dry, and intact, and the uterine fundus was nontender and firm below the umbilicus. Speculum examination revealed scant lochia, and bimanual examination was negative for pelvic tenderness or masses. A rectal examination was performed, and hard stool was palpated throughout the rectal vault.
Laboratory evaluation revealed mild leukocytosis (13.8×106/μL), normal urinalysis, and normal serum electrolytes. Diagnoses considered at this point included constipation, urinary tract infection, nephrolithiasis, appendicitis, and puerperal endometritis. Because the clinical findings were nonspecific and a definitive diagnosis was lacking, she was admitted for further observation and evaluation. Intravenous hydration, pain medication, and ceftriaxone were initiated empirically.
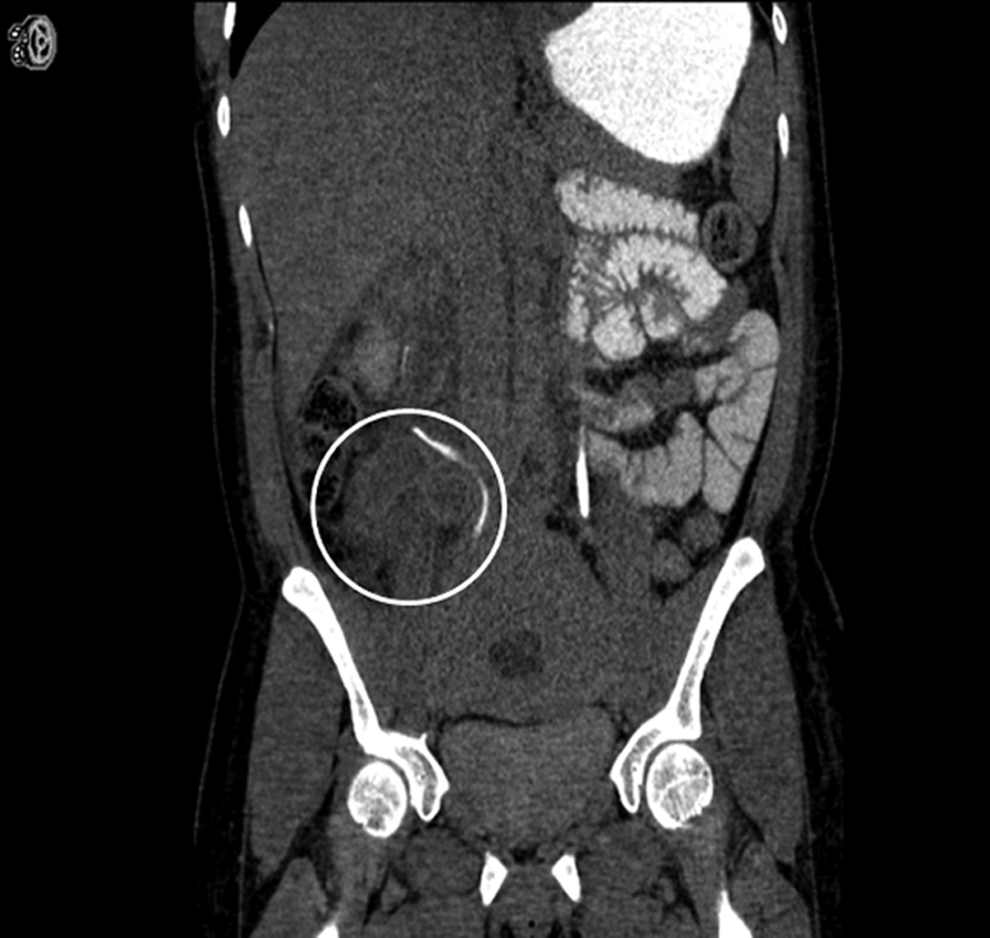
On hospital days 1 and 2, the patient continued to experience right flank pain despite pain medication and adequate intravenous hydration. Her serum creatinine levels increased from 0.64 to 1.01 mg/dL and 1.12 mg/dL on days 1 and 2, respectively. Computed tomography (CT) scan of the abdomen/pelvis with oral and intravenous contrast enhancement revealed an inflamed, serpiginous, peripherally enhancing tubular structure measuring ∼3 cm, extending from the medial aspect of the right kidney to the inferior edge of the right adnexa (Fig. 1). The structure was found to externally compress and displace the right ureter, causing mild-to-moderate hydronephrosis (Fig. 2). The left kidney and ureter were normal. Radiologic findings suggested an acutely thrombosed and distended right ovarian vein. The degree of right hydronephrosis raised suspicions of ureteral obstruction that warranted cystoscopy and retrograde pyelography. These studies revealed midureteral deviation and dilation of the proximal right ureter consistent with obstruction. A double-J ureteral stent was placed under fluoroscopic guidance to relieve the ureteral obstruction.

Peripherally enhancing tubular structure (white circle).
Structure compressing right ureter (white circle).
Results
On hospital day 3, following double-J ureteral stent placement, the patient felt much better and required only minimal use of oral pain medication. Her serum creatinine level decreased to 0.69 mg/dL. She was started on therapeutic enoxaparin, tamsulosin, and ceftriaxone and was discharged on hospital day 5. She continued her enoxaparin for 7 more days and reported no problems on follow-up urologic and gynecologic visits 2 weeks later.
Discussion
Ovarian vein thrombosis is classically known to occur postpartum but may also occur as a complication of pelvic inflammatory disease, malignancy, pelvic surgery, and, rarely, abortion.1,2 Patients with POVT most commonly present with fever, abdominal or pelvic pain, and, sometimes, a palpable sausage- or rope-like abdominal mass.1,2 However, as this case illustrates, some patients present with nonspecific clinical symptoms. As a result, a long list of gynecologic and nongynecologic differential diagnoses is generated, including endometritis, pelvic inflammatory disease, adnexal torsion, adnexal abscess, broad ligament hematoma, urinary tract infection, acute appendicitis, intestinal volvulus, diverticulitis, and perforated ulcer. 2 Often, POVT is not considered until a patient's fever remains unresponsive to antibiotics. 2
Pregnancy and the immediate postpartum period are associated with increased risk of thromboembolic events.1–3 This phenomenon is explained by Virchow's triad: blood flow stasis, hypercoagulability, and endothelial injury.1–3 The diameter of the ovarian vein is up to three times greater at term than in the nonpregnant state, with blood flow sharply declining immediately after delivery. 1 This causes partial collapse of the ovarian veins and may create venous stasis. In addition, venous stasis occurs because the gravid uterus compresses the inferior vena cava and pelvic veins. 3 A relatively hypercoagulable state occurs during pregnancy as a result of decreased protein S levels, decreased fibrinolytic activity, and increased levels of factors VII, VIII, and X.1–3 The exact mechanisms of blood vessel injury have been difficult to elucidate, but the cause is thought to be infectious. 1 Ovarian veins have elaborate communications with uterovaginal venous plexuses, thereby providing an infectious portal of entry. 2 Consistent with this case, it is interesting to note that the right ovarian vein is involved in 90% of POVT cases.1,2 Retrograde drainage from the left ovarian vein and anterograde flow into the right ovarian vein, particularly in the presence of endometritis, may expose the right ovarian vein to a higher bacterial inoculum, explaining this lateralization of POVT.1,2 In addition, uterine dextrorotation results in increased stasis in a longer right ovarian vein, with less competent valves creating a nidus for thrombus formation. 2
As with this patient, only a handful of cases of patients with POVT presenting with urologic problems or complications have been reported in the literature.4–7 The left ureter is not typically obstructed by ovarian vein thrombosis, as it does not cross the left ovarian vein, whereas on the right, the ovarian vein crosses the ureter at the L4 vertebral level.1,2,4–7 Ureteral obstruction secondary to POVT can sometimes manifest with right flank pain and mild elevation in serum creatinine levels, in addition to abdominal pain, fever, and leukocytosis.1,2,4–7 Urinalysis results are typically normal and patients generally do not report urinary symptoms.4–7 The patient presented here had similar clinical symptoms and laboratory findings.
Radiologic imaging has replaced surgery as the diagnostic tool of choice, although surgical exploration may be necessary when radiologic imaging is nondiagnostic and the patient remains febrile despite adequate antibiotics.2,8 In a study by Kubik-Huch et al., 8 for diagnosing POVT, the sensitivities and specificities of ultrasound, CT, and magnetic resonance imaging with angiography (MRA) were 55.6% and 41.2%, 77.8% and 62.5%, and 100% and 100%, respectively. Although MRA was superior to CT scanning, the latter is often the diagnostic modality of choice because it is readily available at most institutions. 8 Although this patient's initial CT scan suggested an acutely thrombosed right ovarian vein, additional sonographic and Doppler imaging ruled out retroperitoneal hematomas or adnexal torsion.
Although clinical manifestations of POVT vary, treatment regimens generally consist of broad-spectrum antibiotics and anticoagulation. Therapeutic anticoagulation should be started only after POVT is confirmed radiologically. 2 Most experts recommend continuing intravenous antibiotics for 48–72 hours and anticoagulation for 7–10 days after fever resolves.1,2 In the setting of ureteral obstruction, as with this patient, standard antibiotic and anticoagulation therapy must be supplemented with a modality to relieve obstruction. This may take the form of double-J ureteral stents, nephrostomy tubes, or, most radically, nephrectomy, in the setting of kidney rupture. 4
Conclusions
POVT is an uncommon cause of abdominal pain in the postpartum patient. POVT complicated by ureteral obstruction is even less common, but should always be considered as part of an already broad differential diagnosis, because the consequences, including pulmonary embolism and kidney rupture, are potentially lethal. Subtle clues that may suggest ureteral obstruction include flank pain and mild elevation in creatinine levels. These are by no means definitive, and clinical suspicion must be supplemented with CT imaging to identify ureteral obstruction. It is postulated that such an approach may lead to prompt diagnosis and treatment, and thereby avoid associated morbidity and mortality.
Footnotes
Disclosure Statement
No competing financial interests exist.