
Abstract
Abstract
Introduction
Cases
During a period of 2 years (2009–2011), 3 pregnant women with acute cholecystitis were treated.
Case 1
A 25-year-old pregnant woman at the 38th week of gestation presented with right upper quadrant abdominal pain with characteristics of biliary colic and fever. Chills or jaundice were not present. Physical examination revealed a gravid uterus appropriate for gestational date, and abdominal tenderness. Laboratory tests, including complete blood cell count, electrolytes, amylase, and liver function tests revealed leukocytosis. Ultrasonographic findings revealed acute cholecystitis and cholelithiasis. Conservative treatment, including intravenous hydration, analgesics (paracetamol), and antibiotics (second generation cephalosporin) was selected. The patient responded well. She was scheduled for laparoscopic cholecystectomy immediately after cesarean delivery, once the episode of cholecystitis had subsided.
Case 2
A 30-year-old pregnant woman at the 38th week of gestation was admitted to the emergency surgical ward with complaints of right upper quadrant abdominal pain resembling biliary colic. She also had fever, but no chills or jaundice. She reported a previous episode of acute cholecystitis in the 26th week of gestation, which had been managed conservatively. On physical examination, there was a gravid uterus appropriate for gestational date, and abdominal tenderness. The patient's hematologic and biochemical profile were within normal limits, except for leukocytosis. She was subjected to ultrasonographic examination, which showed acute cholecystitis and cholelithiasis. Conservative treatment, including intravenous hydration, analgesics (paracetamol), and antibiotics (second generation cephalosporin), followed, but the pain recurred. She was urgently submitted to cesarean delivery and laparoscopic cholecystectomy immediately afterwards.
Case 3
A 31-year-old pregnant woman, in the 39th week of gestation, presented with severe pain in the right upper quadrant, nausea, and vomiting. Neither fever, chills, nor jaundice was present. Abdominal examination revealed a gravid uterus appropriate for gestational dates. Laboratory tests, including complete blood cell count, electrolytes, amylase, and liver function tests were within normal limits except for leukocytosis. Abdominal ultrasonography revealed acute cholecystitis and cholelithiasis. The patient was given conservative treatment, including intravenous hydration, analgesics (paracetamol), and antibiotics (second generation cephalosporin), and she responded well to it. She was scheduled for laparoscopic cholecystectomy immediately after cesarean delivery, once the episode of cholecystitis had subsided.
Operative technique
All women were placed in the supine left lateral tilt position under general endotracheal anesthesia. The caesarean section was performed successfully in all cases through a Pfannenstiel incision. Three healthy infants were delivered: (1) 3540 g; (2) 3300 g: and (3) 3689 g, respectively. The laparoscopic trocar at the umbilical site (10 mm) was placed under direct vision to avoid injury of the still-enlarged uterus (Fig. 1). Hysterotomy repair followed, and the pneumoperitoneum was established at a pressure of 12 mm Hg. The other three (one 10 mm and two 5 mm) trocars were inserted at their standard position. Laparoscopic cholecystectomy was then performed typically (Fig. 2). Irrigation and suction of blood clots was performed in the entire operative field (Fig. 3). The mean time of the operations was 1 hour and 30 minutes (range 1–3 hours).

Laparoscopic trocar at the umbilical site.
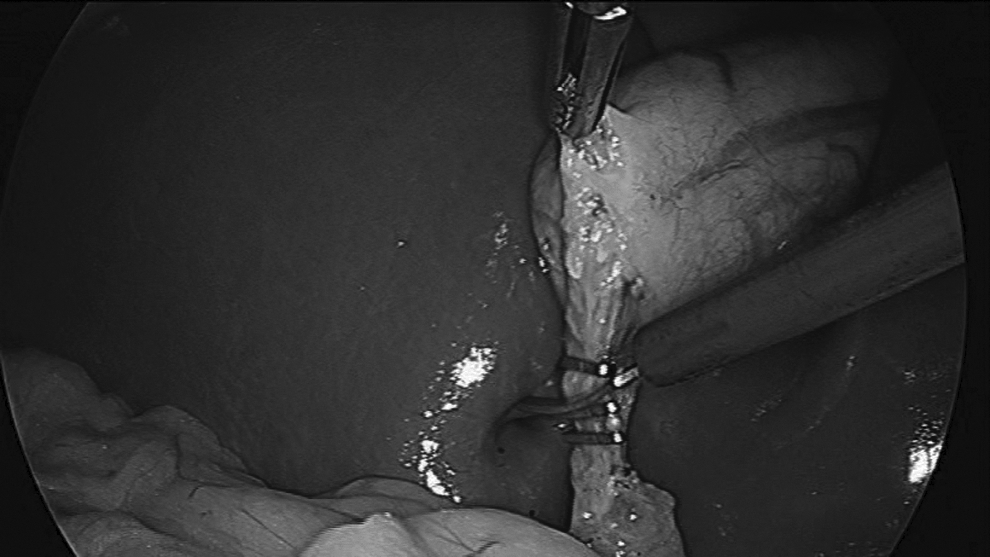
Ligation and division of cystic duct.
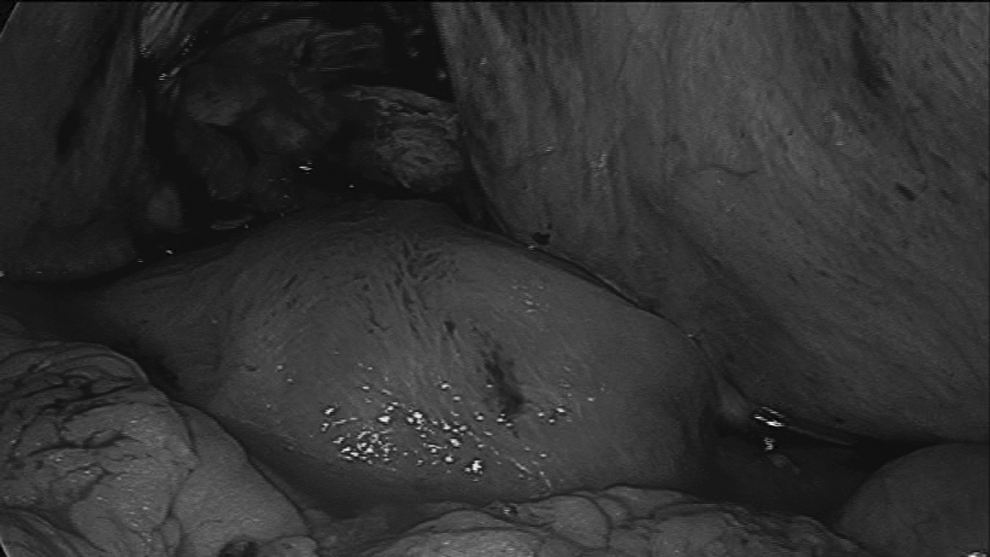
Irrigation and suction of blood clots were performed in the entire operative field.
Results
No major or minor postoperative complications in the mothers or infants were observed. The mean length of stay was 4 days (range 3–5 days). Histologic examination was, in all cases, consistent with chronic cholecystitis.
Discussion
Acute cholecystitis is common during pregnancy, with a frequency of 1–6 per 10,000 pregnancies. 3 Initial treatment is conservative, including intravenous analgesics and antibiotics, in an attempt to avoid surgical intervention during pregnancy. However, these conditions tend to persist frequently, making surgical treatment inevitable. 4
Laparoscopic cholecystectomy has become the procedure of choice for most cases of symptomatic cholelithiasis. The Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) has published specific guidelines, making laparoscopic cholecystectomy a safe, effective, and definite treatment for symptomatic cholelithiasis during the second trimester of pregnancy.5,6
However, even if the episode of acute cholecystitis subsides with conservative therapy, surgery should be performed after delivery.2,7,8 Additional surgery has been used to treat conditions such as appendicitis, adhesions, hernia, and adnexal benign disease at the time of caesarean delivery. This fact led to the suggestion that cholecystectomy can also be safely performed immediately after caesarean delivery.9–12
Open cholecystectomy performed at the time of cesarean delivery would require two incisions or an extended single one, because of the distance between the gallbladder and the uterus. However, this is unfavorable in terms of morbidity, length of stay, and cosmetic result. 7
The laparoscopic approach, however, appears to lack these disadvantages. In the cases reported here, laparoscopic cholecystectomy was performed immediately after cesarean delivery. The infant delivery decreased the size of the uterus, putting it away from the surgical field. Moreover, the laparoscopic trocars were placed under direct vision, which guaranteed their safe entry.
By this means, laparoscopic cholecystectomy was performed safely, efficiently, and rapidly, offering a definite treatment. The patients had no dietary restrictions and, consequently, there was no effect on breastfeeding. The recoveries were uncomplicated, with better cosmetic results, short lengths of stay, and reasonable costs.
Conclusions
The current authors' experience confirms that laparoscopic cholecystectomy immediately after caesarean delivery is an attractive and successful approach for both general/obstetric surgeons and patients.
Footnotes
Disclosure Statement
No competing financial interests exist.