
Abstract
Abstract
Introduction
I
Case
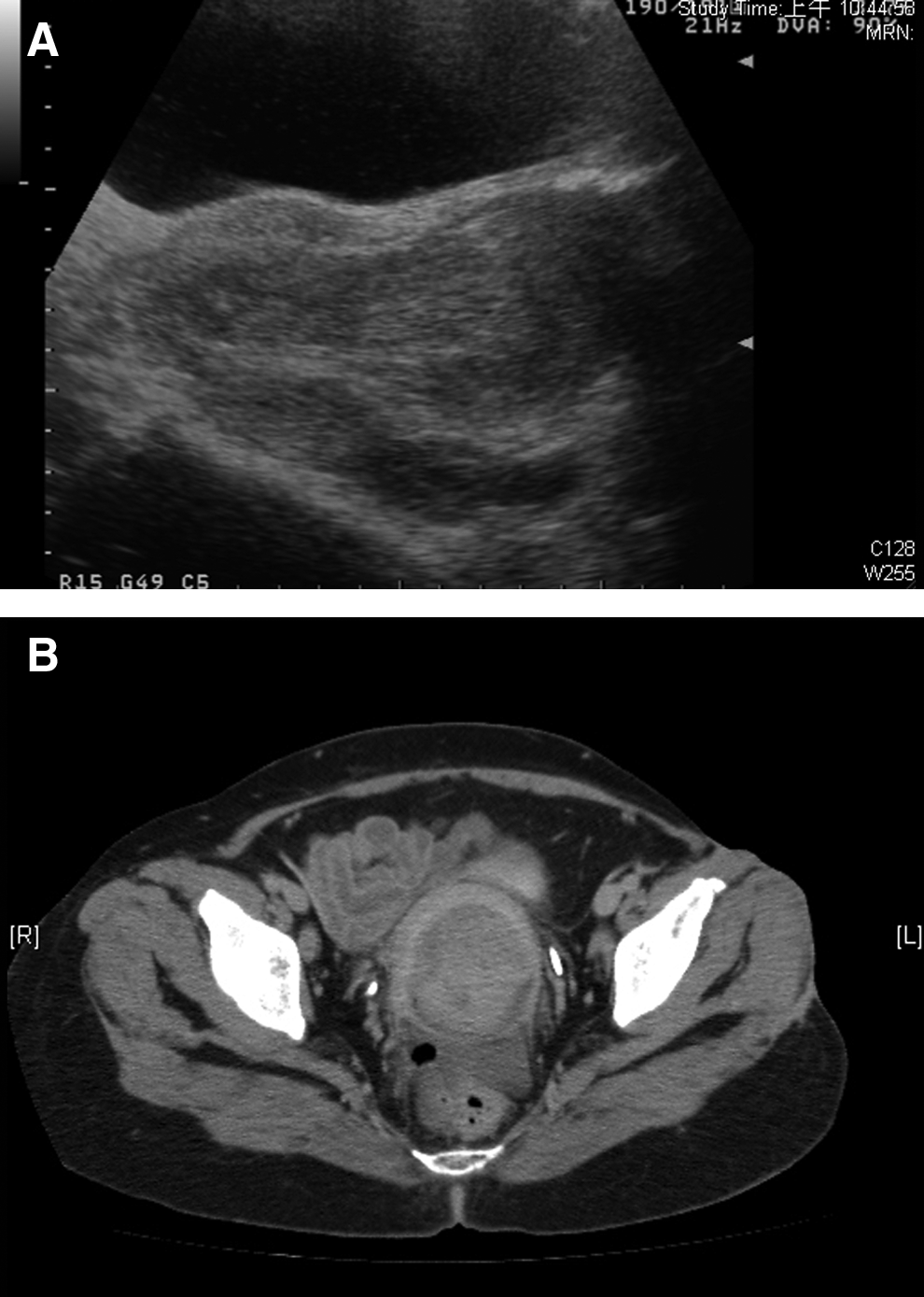
A 38-year-old woman, gravida 3, para 2, presented with persistent vaginal bleeding and lower abdominal pain for the past year. More recently, the patient had noted that she had a malodorous vaginal discharge. She reported also having dysuria, urgency, increased urinary frequency, and nocturia. Her past surgical, gynecologic, and medical histories were unremarkable. She was pale and ill-looking and she had mild lower abdominal tenderness. A vaginal examination showed a 10-cm round leiomyoma protruding into her vagina. Hemorrhagic areas were also noted. Her cervix was not visible and her uterine fundus was not palpable. Laboratory data indicated anemia (a hemoglobin concentration of 5.1 mg/dL). This patient received 3 units of packed red blood cells. A chest X-ray did not reveal any specific findings. Abdominopelvic computed tomography (CT) and transabdominal ultrasound were performed and they showed a large submucosal uterine leiomyoma (Fig. 1). Uterine inversion was suspected. After signing an informed consent form, the patient underwent a laparotomy, via a Pfannenstiel incision. During the surgery, no uterine structure was identified. There was only one constriction ring at the normal uterine site (Fig. 2). Her Fallopian tubes were traced centrally to a concave, umbilicated fundus, and uterine inversion was recognized. Afterward, a Haultain procedure was successfully performed, via an incision on the full thickness of the posterior wall of her uterus, up to the constriction-ring level. Her fundus was repositioned, and an abdominal hysterectomy was performed. Both ovaries were viable and were thus preserved. The final pathologic report revealed a myomatous nodule, measuring 9×8.8×8.7 cm with areas of hemorrhage and degeneration (Fig. 3).

Classic laparotomy view, with a well-defined constriction ring.

Results
During the postoperative period, the patient developed a complicated wound infection and was discharged only 18 days after the surgery. Findings on subsequent follow-up examinations were unremarkable.
Discussion
Nonpuerperal inversion of the uterus is an extremely infrequent condition, and it is almost always associated with a prolapsed uterine tumor. In the literature, since 1887, there have been ∼150 cases described, and the majority of them were caused by benign tumors, namely leiomyomas. 2 The remaining cases of tumor-induced inversion were uterine sarcomas.2–8
In general, nonpuerperal uterine inversion presents after 45 years. Usually, the most common complaints associated with uterine inversion are abnormal vaginal bleeding and low abdominal pain. However, patients may present with additional symptoms, such as vaginal discharge, anuria, and a protruding mass from the vulva. 3
The definitive etiology of uterine inversion is not clearly understood; however, one possible mechanism of action may be that a tumor distends the cavity and consequently irritates the uterine wall, which, in turn, contracts in an attempt to expel the tumor.4–6 Other proposed events that may lead to inversion of the uterus include: a thin uterine wall; rapid growth of a tumor; tumor size; fundic localization of the tumor and a tumor attached to the uterine wall by a thin pedicle4–6
Because of its rarity, uterine inversion is difficult to diagnose, but there are two major clinical hallmarks for making a correct diagnosis: (1) an impalpable uterine fundus and (2) an invisible cervix. Pelvic ultrasonography may be a useful tool for diagnostic purposes and may also facilitate the operative performance. 3 In the current patient, both the sonogram (showing poor delineation of the endometrial lining) and the CT scan were useful for the presumptive diagnosis; however, magnetic resonance imaging (MRI) is probably the best technology for diagnosis. 8
Treatment of uterine inversion is surgical—either vaginal or abdominal hysterectomy. Focusing on the vaginal approach, the described procedures include opening the anterior (Spinelli) or the posterior (Küstner) vaginal wall. Both of these interventions are not easy because the vagina is usually filled with the protruding tumor and with the uterus.3–5 Two abdominal techniques have been described by Huntington and Hultain. For the Huntington procedure, the inverted portion is pulled from the uterus. However, this is unsuccessful in most cases because of the strong constriction ring. 4 The Hultain procedure involves incising the full thickness of the posterior uterine wall to achieve a normal anatomy. This is a safe and effective way to reposition the fundus, particularly in nononcologic cases. 4
Conclusions
The current case had several issues that made it quite interesting. According to the literature, generally, nonpuerperal uterine inversion presents after 45 years and is mostly associated with benign leiomyomas and seldom occurs with uterine malignancies.2,6 Thus, this case is one of the few of a uterine inversion in a reproductive-age woman. Another fact that contributes to the uniqueness of this case is the surgical result. Although the patient had a complete uterine inversion, the ovaries were traced and viable and, thus, were possible to preserve.
This condition presents a challenge, mainly because of the unusual clinical, imaging and operative findings involved.
Footnotes
Disclosure Statement
No competing financial conflicts exist.