
Abstract
Abstract
Introduction
A
In this case, an intramyometrial uterine cyst, its histologic and immunohistochemical description, and a review of recent literature are presented.
Case
A 57-year-old female patient, who was a smoker, presented with autoimmune hepatitis that had evolved for 10 years without treatment. In a control abdominal ultrasound for her autoimmune hepatitis, a simple cystic formation of 3.5 cm located in the right iliac fossa was found, giving the impression of being a simple cyst. Her previous surgery consisted of an appendectomy, tubal ligation 16 years previously, and surgery for carpal tunnel syndrome. She had given birth twice; one through natural childbirth 30 years earlier, and once through cesarean delivery 34 years earlier. She had been postmenopausal for 3 years, and she had been treated with hormone-replacement therapy consisting of estradiol valerate 2 mg, plus dienogest 2 mg, for 2 years. Previously, she had had no symptoms and her menstrual cycles had been normal.
In a magnetic resonance imaging (MRI) study (Fig. 1), there was a round lesion 3.6×3.3 cm in diameter in the pelvis, which showed cystic characteristics, with a homogeneous low signal on T1-weighted sequence and a homogeneous high signal on T2-weighted sequence, which, after intravenous contrast administration, showed a subtle enhancement of the wall. A computed tomography (CT) scan of the abdomen (Fig. 2) in contrast, showed the same lesion of 4.2×3.7 cm located at the level of the mesenteric fat in the pelvic region. Figure 3A–D shows images of the CT scan, with the relationship between the uterus and the uterine cyst.

Cystic lesions revealed on magnetic resonance imaging in T1.
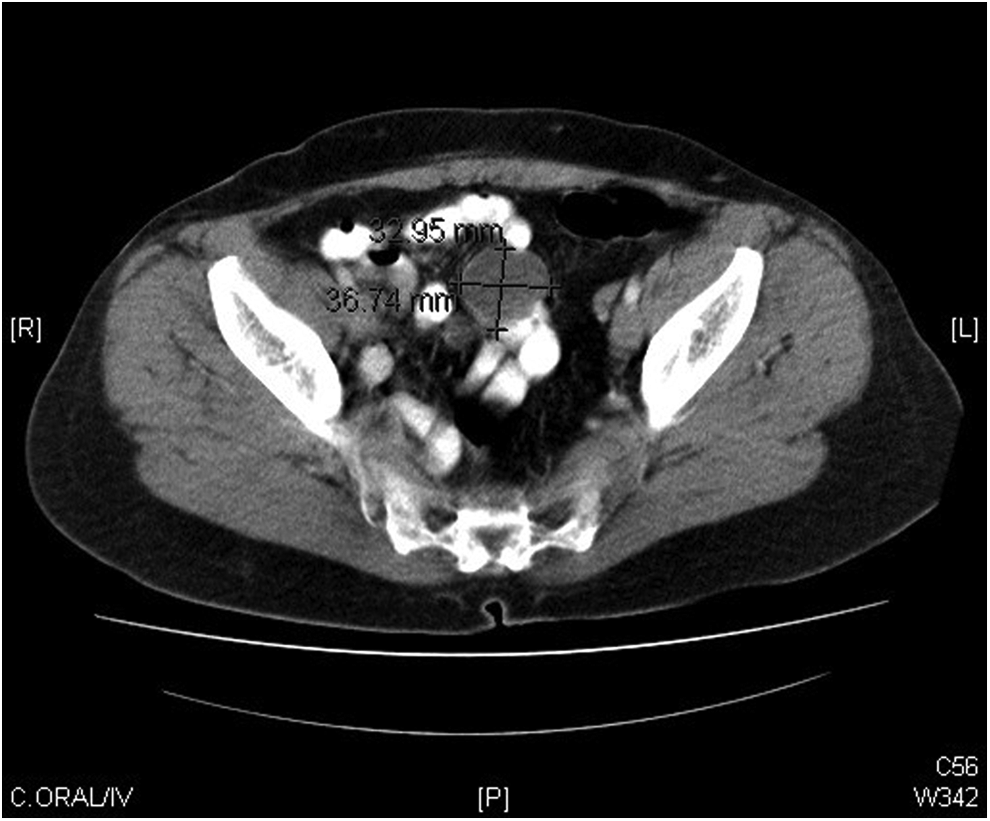
Cystic lesion shown on computed tomography with contrast.
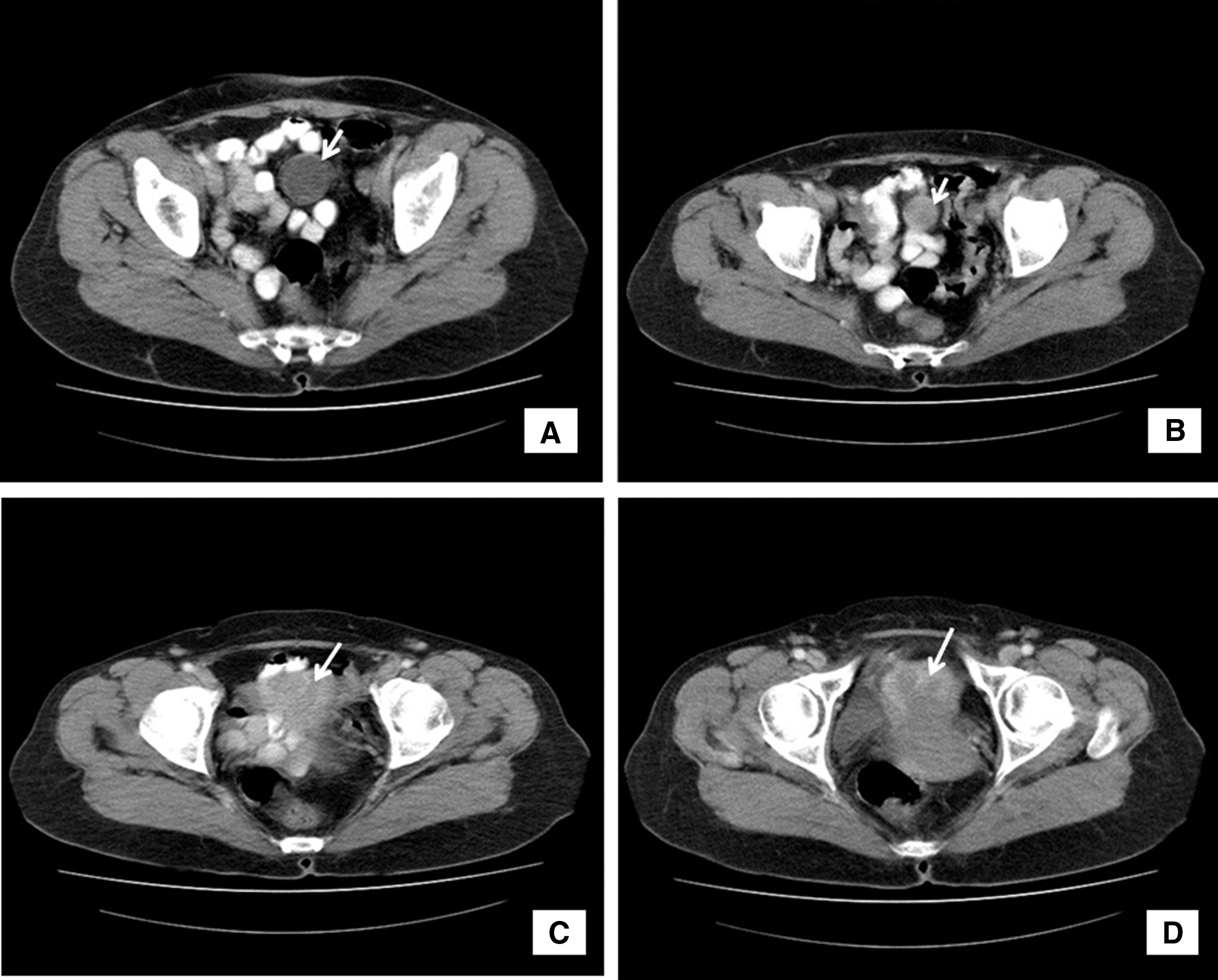
Computed tomography shows the relationship between the uterus and the uterine cyst.
Given the findings, and it being impossible to rule out associated malignancy, it was decided to undertake complete removal of the lesion and have a histologic analysis of the excised material.
Results
An infraumbilical midline laparotomy was performed, with complete removal of a smooth wall and translucent brownish cystic lesion located at the midline of the uterine dome. It contained ∼4 mL of clear liquid without sediment, and there was no evidence of thickening or partitioned areas inside.
The patient underwent an enucleation of the cystic mass without hysterectomy.
When histopathology testing was performed on the postsurgical specimen, macroscopic findings showed a cystic formation measuring 2.3×2.1 cm and having external and internal brown and smooth walls, whose content was ∼4 mL of a clear liquid without sediment. There was no observable connection between the endometrial cavity and the cyst cavity. Upon microscopic study, a cystic lesion with ciliated wall lining, without atypia, and with myometrial smooth muscle thickened with congested vessels, was observed. Sometimes the epithelium has intraluminal projections. No basement membrane was identified nor did PAS [periodic acid-Schiff testing] identify any positive intraepithelial cells (Fig. 4A and B). In immunohistochemical analysis, the cyst lining cells expressed cytokeratin (CK) AE1/AE3, whereas calretinin and CD-10 were negative (Fig. 4C).

There were no other gross pathologic findings in her other abdominal organs. She was discharged without any incidents on the fourth day postsurgery.
Discussion
A uterine or intramyometrial cyst is a benign lesion, and is extremely rare. The first reference to intramyometrial cyst was made by Atlee in 1850. 4 Subsequently, very few cases have been described, and even fewer are accompanied by histopathologic description. 1
The histopathologic description of congenital uterine cyst defines it as a cystic structure, formed by a benign columnar ciliated cuboidal epithelium, without the presence of endometrial stroma, and myometrium surrounded by muscle. 2
Uterine cysts are classified as congenital or acquired. 1 The differential diagnosis should include congenital cysts; cysts of the Wolffian and Müllerian duct that are distinct from those that are acquired; adenomyosis; cervical Nabothian cysts; cystic degeneration of an intrauterine leiomyoma; cystic degeneration of an adenomatoid tumor, an adenocystic tumor, or an accessory, cavitated uterine mass, or intramyometrial hydrosalpinx; and cysts of parasites, such as hydatid cysts.4–11
It is important to differentiate cystic adenomyoma of the uterus, which appears as the most common intramyometrial cyst and presents, unlike uterine cysts, as glandular and endometrial stroma in the wall. 12
Cystic degeneration of the adenomatoid tumor is extremely rare, with subserosal location in the posterior of the uterine fundus or near the Fallopian tubes. Likewise, immunohistochemical techniques can differentiate congenital uterine cysts and cystic adenomatoid tumor, as the latter shows immunopositivity for cytokeratin and calretinin. 13
Nabothian cysts are mucous retention cysts, covered by cylindrical endocervical epithelium. 6
It is also important to differentiate the accessory, cavitated uterine mass, which has as diagnostic criteria: (1) an isolated accessory cavitated mass; (2) a normal uterus (endometrial cavity) and normal Fallopian tubes and ovaries; (3) surgery required to excise the mass, with pathologic examination postsurgery on the excised mass to confirm its nature; (4) an accessory cavity lined by an endometrial epithelium with glands and stroma; (5) chocolate-brown–colored fluid content; and (6) no adenomyosis (if the uterus is removed), although there could be small foci of adenomyosis in the myometrium adjacent to the accessory cavity. 11 These criteria are unlike the histopathologic description of a congenital uterine cyst that is defined as a cystic structure, formed by a benign columnar ciliated cuboidal epithelium, without the presence of endometrial stroma and myometrium surrounded by muscle. 2
The intramyometrial hydrosalpinx is characterized by a true cyst lined by a tube-type epithelium, 5 and, in the current case, the Fallopian tubes had no macroscopic abnormalities and there was no tubelike epithelium noted in the histopathologic description.
A congenital uterine cyst usually contains clear fluid within it; a Müllerian cyst is usually located in the midline, whereas the one derived from the Wolffian duct is usually located on the sides of the uterine wall. A Müllerian cyst also lacks a basement membrane, and has columnar or cuboidal epithelial cells, often with villi, whereas the Wolffian cyst does not contain mucin, has a cuboidal or columnar epithelium lacking villi, and does not respond to hormonal stimulation. 13
There are a number of criteria for the diagnosis of congenital uterine cyst, described by Sherrick and Vega. 1 The first is that the cyst should not communicate with the uterine cavity or with the line of the endometrial epithelium. Second, it should be formed by a cuboidal or columnar epithelium with or without cilia, differing in that, if it has a low papillary epithelium, it resembles a Müllerian cyst, whereas, if the epithelium is of a smooth type, it appears like like a cyst derived from the Wolffian duct. The third criterion is that the cyst must be located in the myometrium and partially composed of the myometrium tissue. 1
The histopathologic examination in this case shows a cystic structure, containing a clear liquid inside, consisting of ciliated cylindrical epithelium without atypia, which has no basement membrane and is lined by myometrium—a structure that resembles a congenital Müllerian cyst.
The etiopathogenesis of uterine cysts is not clearly determined, although several hypotheses exist. The theory explains the origin of congenital cyst as a disturbance during the embryonic development of the female urogenital tract, with cysts that arise from the Wolffian or Müllerian epithelium. In contrast, the acquired theory, applicable to acquired cysts, defines the origin of the intramyometrial cyst of the adenomiotic uterus, which may arise from intrauterine manipulations, such as endometrial ablation or cesarean delivery.1–3,14,15
In the histologic study of the case presented, there is no epithelium or endometrial stroma, thus presenting a congenital origin, fulfilling the criteria of Sherrick and Vega, 1 showing absence of endometrial communication with a histologic structure, compatible with Müllerian duct cyst, covered, and partly composed of myometrium.
Conclusions
This new case of congenital uterine cyst, with a histopathologic description and immunohistochemical analysis, may enable elucidation of the pathogenesis of this rare disease in the future. Diagnosis of a congenital uterine cyst has complex critera needed to distinguish it from other kinds of cysts.
Footnotes
Disclosure Statement
No competing financial interests exist.