
Abstract
Abstract
Introduction
T
Many studies in the past have demonstrated the role of cyclin D1 in endometrial carcinogenesis. Cyclins are key components in the regulation of the cell cycle in combination with their respective cyclin-dependent kinases (cdks). 2 Cyclin D1 was originally cloned as an oncogene responsible for parathyroid adenomas. 3 Subsequently, the aberrant expression of cyclin D1 was documented in several human malignancies.
The purpose of the current study was to evaluate the expression of cyclin D1 in hyperplasia and endometrial carcinoma to determine the role of cyclin D1 in endometrial carcinogenesis. Another goal was to see the variation of cyclin D1 expression in various tumor types, especially serous and endometrioid carcinomas. The aim was to shed lighton the role of cyclin D1 in the dualistic model of endometrial carcinogenesis. The current authors also attempted to correlate cyclin D1 expression with, grade, stage, and other clinicopathologic parameters in endometrial carcinomas.
Materials and Methods
The present study was conducted in the department of pathology of Pt. B.D. Sharma Post Graduate Institute of Medical Sciences, in Rohtak, Haryana, India, over a period of 2 years. A total of 50 cases, providing 41 hysterectomy specimens and 9 endometrial biopsies, were included in the study. Tissues were routinely fixed in buffered formalin and were paraffin-embedded. Eighteen cases of normal endometrium (36%), 14 cases of simple hyperplasia (28%), 4 cases of complex hyperplasia (8%), and 14 cases of endometrial adenocarcinoma were diagnosed, following established histopathologic criteria reported in the literature. Routine hematoxylin and eosin staining of the sections was performed. Cyclin D1 was evaluated for intensity and extent in each of the cases. Clinicopathologic variables of endometrial carcinoma were correlated with cyclin D1 expression.
Immunohistochemistry was performed by mounting 3–4-μm sections on slides coated with a suitable tissue adhesive. Sections were deparaffinized of xylene and rehydrated through graded alcohols. The slides were then washed in running tap water. Antigen retrieval was performed, using citrate or Tris EDTA [trisaminomethane-ethylenediaminetetraacetic acid] in a pressure cooker or microwave oven. The sections in TBS [Tris-buffered saline] were rinsed, and excess TBS was drained out. Endogenous peroxidase was blocked, using a peroxidase block for 5 minutes. The samples were washed with TBS for 5 minutes and were incubated with a protein block for 5 minutes. The samples were again washed in TBS. Optimally diluted primary antibody was applied for 60 minutes. Once again, the samples were washed in TBS. They were then incubated with a postprimary block for 30 minutes and washed again in TBS. They were then incubated in DAB [3, 3'-diaminobenzidine] solution for 10 minutes. The slides were then rinsed in TBS and transferred to running water. Counterstaining was performed with hematoxylin, and dehydration was performed with graded alcohols and xylene. Counterstaining was performed again with hematoxylin, and dehydration was performed again with graded alcohols and xylene. The samples were then cleared and mounted in DPX [di-n-butyl phthalate in xylene].
Cyclin D1 positivity was seen as brown-to-blackish nuclear staining. Positive and negative controls were run simultaneously. Tonsil epithelium was chosen as a positive control. A negative control was creating by substituting the primary antibody with an antibody of irrelevant specificity. For statistical purposes, the intensity and extent of nuclear staining for cyclin D1 was evaluated. Intensity was graded as: 0, no staining; 1+, weak nuclear staining (a faint chromatin pattern); and 2+, moderate nuclear staining (chromatin clearly defined). The extent of staining was graded on a scale of 0–100, and scoring was determined as: cyclin D1 staining <10% of the nuclei=0; 11%–30%=1+; 31%–60%=2+, and 61%–100%=3+. The data collected were statistically analyzed using a Student's t-test and an χ2 test. 4
Results
No cases of simple hyperplasia were positive for cyclin D1 expression. All of the cases of complex hyperplasia and 64.2% cases of carcinoma of the endometrium were positive for cyclin D1 expression (Table 1). The extent of cyclin D1 in various lesions of the endometrium were evaluated. As noted above, none of the cases of simple hyperplasia showed positivity for cyclin D1. Complex hyperplasia showed positivity in all 4 cases, with an extent of 3+ in 1 case (Fig. 1) and 2+ in 2 cases (Fig. 2). Endometrial carcinomas were also analyzed, and 7 (50%) cases were 3+ (Fig. 3), and 2 cases (14%) were 1+ in extent (Table 2). All three groups—simple versus complex (p=0.00), complex versus carcinoma (p=0.002), and simple versus carcinoma (p=0.00)—showed significant differences, per the χ2 test. There was a statistical difference in extent between simple and complex hyperplasia and between complex hyperplasia and endometrial carcinoma. There was also a marked statistical difference between simple hyperplasia and carcinoma of the endometrium.
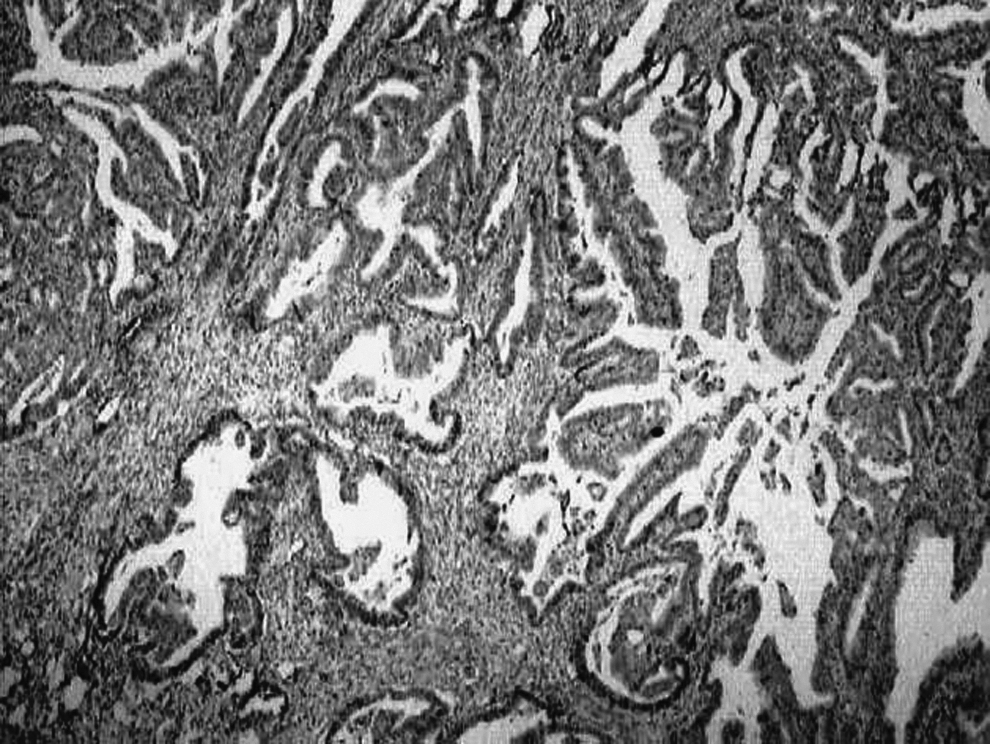
Immunohistochemical staining for cyclin D1 in complex hyperplasia of the endometrium with an intensity of 1+ and an extent of 3+ (40×).

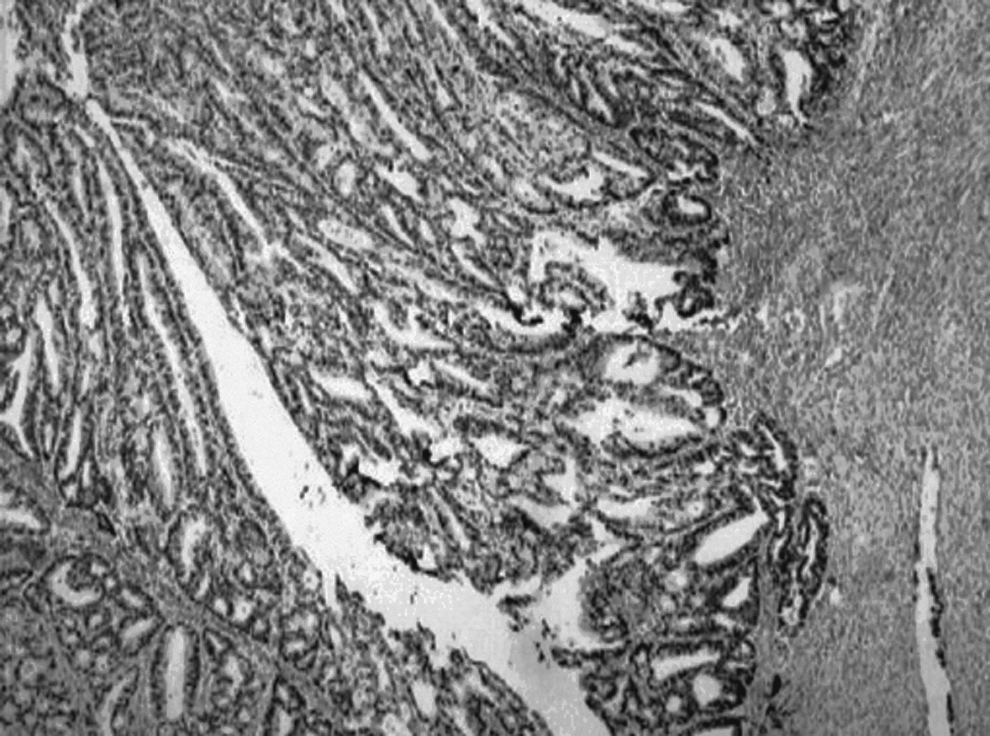
Immunohistochemical staining for cyclin D1 in complex hyperplasia the of endometrium with an intensity of 2+ and an extent of 2+ (400×)
Immunohistochemical staining for cyclin D1 in endometrioid carcinoma, with an intensity of 3+ and an extent of 3+ (40×).
The intensity of cyclin D1 in various lesions of the endometrium was also evaluated. Complex hyperplasia showed positivity in all 4 cases, with an intensity of 2+ in 1 case (Fig. 2) and 3+ in 3 cases (Fig. 1). Endometrial carcinoma had an intensity of 3+ in 7 (50%) cases (Fig. 3) and 2+ in 2 (14%) cases (Table 3). Statistical evaluation also showed no difference in intensity between complex hyperplasia and carcinoma of the endometrium (p=0.369).
Fourteen cases of endometrial carcinoma were classified as: endometrioid, clear-cell, or serous carcinomas. Most cases (64.3%) were endometrioid carcinomas, 3 cases (21.4%) were clear-cell carcinomas, and 2 cases (14.3%) were serous carcinomas. Of 9 cases of endometrioid carcinoma, 6 (66.67%) were positive for cyclin D1. All clear-cell carcinoma cases were positive for cyclin D1 (Fig. 4), but none of the cases of serous carcinoma were positive for cyclin D1.
Clinicopathologic parameters—such as menopausal status, myometrial invasion, histologic grade and International Federation of Gynecology and Obstetrics (FIGO) staging—were correlated with cyclin D1 expression. No statistical differences were found between expression of cyclin D 1 and menopausal status, tumor grade, myometrial invasion, or FIGO stage. This analysis was performed only for cases of endometrioid carcinoma, because fewer cases were available for serous and clear-cell carcinoma.
Discussion
This current immunohistochemical study of cyclin D1 on formalin-fixed, paraffin-embedded tissue sections revealed that cyclin D1 expression was negative in normal endometrium (secretory and proliferative endometrium) and simple hyperplasia. All cases of complex hyperplasia and 9 (64%) of 14 cases of carcinoma were positive for cyclin D1. According to statistical analysis, cyclin D1 immunoreactivity in simple hyperplasia and endometrial carcinoma was significant (p=0.000).
In previous studies, the positivity of cyclin D1 in endometrial hyperplasia ranges from 0% positivity (as reported by Tsuda et al. 5 ) to 83% (as reported by Cao et al. 6 ). Cyclin D1 immunopositivity was also reported to be 0% in simple hyperplasia by Ozuysal et al. 7 Quddus et al. reported cyclin D1 positivity as 57% in simple hyperplasia, 71% in complex hyperplasia, and 68% in endometrial carcinoma. 8 Moreno-Bueno et al. reported a percentage of positivity rate for cyclin D1 expression as 13.8% in endometrial carcinoma, but they did not report cyclin D1 expression in cases of atypical endometrial hyperplasia. 9 Horree et al. explored expression of cell-cycle protein in normal, premalignant, and malignant lesions; the current study showed upregulation of cyclin D1 in endometrial hyperplasia and endometrial carcinoma. 10 Nikaido et al. also investigated the role of cyclin D1 in the development of human uterine endometrial carcinoma. They found restricted expression of cyclin D1 in only a few cells of hyperplastic endometrium, whereas cyclin D1 was preferentially expressed in 40% (30/70) of endometrioid carcinomas. 11 Nishimura et al. found 25% positivity in endometrial hyperplasias and 46.1% positivity in endometrioid carcinomas. 12
The current study had the closest resemblance to a study done by Chaudhary and Bansal, which did not show any expression in simple hyperplasia and showed 50% expression in endometrial carcinoma. 13 The current study showed no expression in simple hyperplasia and 64% in endometrial carcinoma (Table 1). The positivity for complex hyperplasia was more than what occurred in endometrial carcinoma; this was similar to the study done by Quddus et al., who reported 71% positivity in complex hyperplasia, compared to 68% in endometrial carcinoma, 8 suggesting that the dysregulation is maximal in a complex hyperplasia state, and that overexpression of cyclin D1 may be an early event in endometrial carcinogenesis. The current study's findings support the significance of complex hyperplasia as a precursor lesion but do not support the notion that simple hyperplasia is precancerous. The mechanism of cyclin D1 dysregulation in endometrial neoplasia is not well-defined, but it is likely that the dysregulation contributes to an increase in the proportion of cells in transition from G1 to the S phase. Cyclin D1 is a key protein in the regulation of the cell cycle at the G1 to the S-phase transition and is essential for regulation of proliferation, differentiation, and transcriptional control. Overexpression of cyclin D1 induces excessive cellular proliferation and is a feature of a number of cancers, including endometrial neoplasia 3 . Apparently, normal endometrium (secretory and proliferative) and simple hyperplasia do not show excessive cellular proliferation, and cyclin D1 is not expressed in them. Few cases of endometrial carcinoma do not show expression of cyclin D1, suggesting the existence of an alternative pathway in endometrial carcinogenesis and thereby proving that other cell-cycle regulatory protein and genetic alterations are also involved in carcinogenesis.
In the current study, the extent of cyclin D1 in various lesions of endometrium was evaluated. The analysis revealed a statistical difference in the extent of cyclin D1 immunoreactivity between simple hyperplasia and endometrial carcinoma (p=0.00). Quddus et al. 8 and Chaudhary and Bansal 13 also studied the extent of cyclin D1 immunoreactivity in simple hyperplasia, complex hyperplasia, and carcinoma of the endometrium, and found no statistical difference in extent between complex hyperplasia and endometrial carcinoma (p=0.84). However, in the current study, a statistical difference was found in extent between complex hyperplasia and carcinoma of the endometrium (p=0.002). The intensity of cyclin D1 in various lesions of the endometrium was also evaluated. Complex hyperplasia (Table 3) showed positivity in the 4 cases, with an intensity of 2+ in 1 case and 3+ in 3 cases. Endometrial carcinomas showed an intensity of 3+ in 7 (50%) cases and 2+ in 2 (14%) cases. The previous study done by Chaudhary et al. 13 showed that there was no statistical difference in intensity between complex hyperplasia and carcinoma of the endometrium. Statistical evaluation in the current study also showed no difference in intensity between complex hyperplasia and carcinoma of the endometrium (p=0.369). Quddus et al. found similar results in their study. 8
Conclusions
It was inferred that cyclin D 1 expression is a quantitative molecular dysregulation that is increasing progressively in extent from complex hyperplasia to carcinoma of the endometrium. This defines the gene's role in endometrial carcinogenesis as an informative biomarker. The biomarker can be used to recognize subsets of endometrial lesions that may be precancerous, and thus susceptible to surgical therapy. Lesions that may be responsive to hormonal manipulations can be excluded. In the current study, various clinicopathologic parameters—such as menopausal status, myometrial invasion, histologic grade, and FIGO staging—were correlated with cyclin D1 expression. No statistical differences were found between expression of cyclin D 1 with these parameters. In the past, Nikaido et al., 11 Shih et al., 14 and Wu et al. 15 found significant associations of cyclin D1 expression in endometrial carcinoma with various clinicopathologic parameters. The current study included 9 cases of endometrioid carcinoma, which is a small number; therefore, more follow-up studies with larger populations are necessary to determine whether or not cyclin D1 expression is significant in the prognosis of endometrial carcinoma.
Footnotes
Disclosure Statement
No financial conflicts exist.