
Abstract
Abstract
Introduction
Case
A female patient, age 74, was 27 years postmenopause. She had had 2 years of abdominal distension, and for 2 days prior to presentation she had noted having an abdominal mass. On February 27, 2012, she was admitted to the hospital.
This patient had lower abdominal distension and a palpable circular mass of ∼25×15 cm in size. The upper edge of the mass was two fingers below her navel, and the lower edge of the mass reached 1 cm beyond her symphysis pubica. The right and left sides of the mass were close to the anterior axillary line. The texture of the mass was rigid, without cystic fluctuations. The mass had poor mobility, was not tender, and did not produce rebound tenderness nor a vascular murmur. A gynecologic examination showed that the vulvovaginal appearance was essentially normal with cervical atrophy. Palpation of her uterus and double annex were not satisfactory because of the presence of the lower abdominal mass. The relationship between the mass and uterus was not clear.
The results of routine blood and urine tests—α-fetoprotein, CA-125, and lactate dehydrogenase levels—were normal. A full set of female hormone tests produced normal results for a person who had changes in hormone levels as a result of menopause. Her CA-19-9 was 85.050 U/mL and her carcinoembryonic antigen was 3.320 ng/mL. A 64-slice spiral computed tomography (CT) scan (Fig. 1) showed a huge cystic mass in the bladder, above the uterus. The mass had a clear edge with a size of 11.9×17.6×14.9 cm and a smooth cystic wall. There were punctate calcifications within or below the cystic wall. Punctate calcifications produced a slightly higher-density shadow. No abnormality was observed after enhancement. This patient's uterus, bladder, and adjacent bowels were displaced because of the pressure of the cystic mass. Her pelvic lymph nodes were not enlarged. However, examinations indicated huge cystic occupation in her pelvis, ovarian cystadenoma, or ovarian teratoma. Ultrasound examination (Fig. 2) showed an anterior positioning of her uterus, with a size of 29×15×35mm. No obvious mass acoustic imaging was observed. Both ovaries were unclear. A cystic mass with a size of 169×94×114 mm was palpable in her pelvic cavity. The boundary of the mass was clear, the capsule of the mass was complete, and the sonolucent area was poor. Many light spots and spot floating were observed, indicating a teratoma of her ovary.
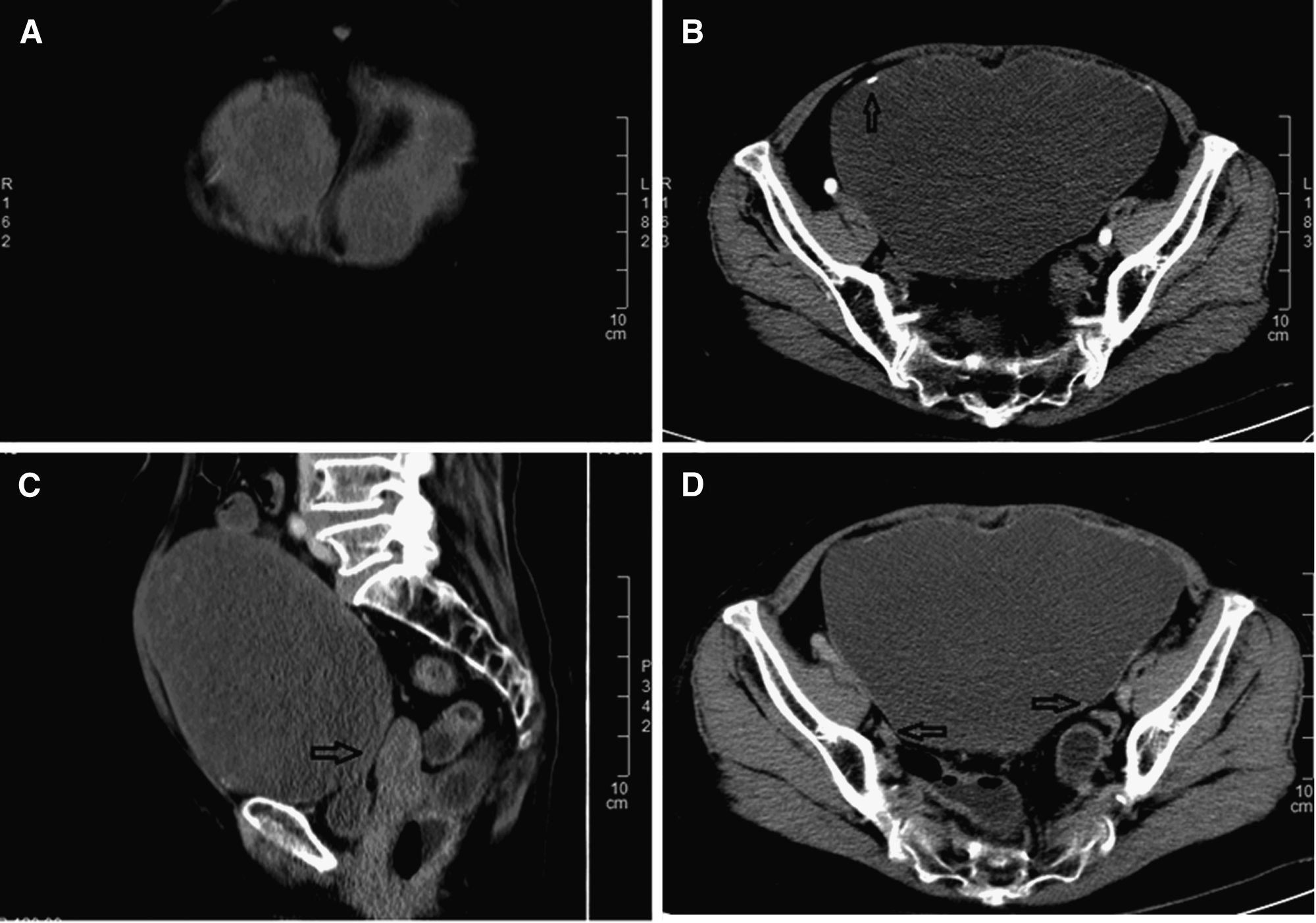
Computed tomography scan images

Ultrasound examination. Many light floating spots were observed.
After preoperative preparation, a laparotomy was performed under continuous epidural anesthesia on March 1, 2012. Skin and subcutaneous incisions was performed, the rectus sheath was cut open, and blunt dissection of the rectus abdominis was performed. There was a large amount of thick, grayish-yellow “greaselike” liquid overflow. The liquid was absorbed and a huge cystic cavity with a size of 20×17×6 cm was revealed. The cystic wall was rough, but obvious papillae were not observed. A quick pathologic examination of the cystic wall indicated a mature teratoma. There were approximately 1500 mL of cystic content. The cyst was rinsed with a large amount of normal saline; no multilocular cyst was noted. The cystic wall was closely connected with the surrounding tissue. After complete peeling of the cystic wall, the cyst was found between the rectus sheath and parietal peritoneum (also called the preperitoneal space). The structure of the parietal peritoneum and rectus sheath was complete without tumor invasion. The peritoneum was cut open for abdominal exploration. The surface of the liver, gallbladder, stomach, intestine, omentum, uterus, and attachments were smooth. No masses or adhesions were observed in these organs. A drainage tube was placed, but no special liquid was drained. Postoperative pathologic examination of the preperitoneal space indicated the presence of a mature cystic teratoma.
Results
This patient recovered well and was discharged 7 days after her operation.
Discussion
The preperitoneal space is located between the inner layer of the peritoneum and the outer layer of the transverse fascia. 1 In the case described above, the volume of this patient's mature teratoma was derived from preperitoneal space but not from the abdominal organs. The teratoma was huge and, to the current authors' knowledge, this kind of case has not reported prior to the current case.
Reports of other teratomas
There were 2 cases of abdominal-wall malignant teratomas and fetal teratomas reported previously,2,3 but the exact anatomical level of the abdominal-wall involved was not described in detail. Teratomas located in the adipose tissue of the abdominal wall and paraumbilical rectus abdominis,4,5 or abdominal-wall metastases of malignant teratoma have been occasionally reported.6–9
Reasons for misdiagnosis
Rare locations of tumors
In this patient, the teratoma had an expansive growth in the preperitoneal space. Because this space is large and distant from the pelvic organs, tumor growth is not restricted and early symptoms may not emerge. Only when the tumor is expanded to a large extent, are abdominal distension and mild discomfort likely to occur. In addition, the midline of the body is occupied by the rectus, and lobular performance was reflected in body and imaging examinations.
Elevation of serum content of CA-19-9 (85.05 U/mL)
CA-19-9 is mainly distributed in normal fetal tissues, while very little content is present in adult sera. Studies have shown that CA-19-9 level is elevated in the sera of patients with ovarian mature teratomas. 10 A positive rate of CA-19-9 is 55.7%, ranging from 39.6% to 86% in different reports. The level of CA-19-9 is positively correlated with the diameter and weight of a mature ovarian teratoma. Therefore, CA-19-9 can be used as a marker for diagnosing mature teratomas.11,12
Compression of pelvic organs leads to the misdiagnosis of pelvic tumors
Ultrasound examination has limitations because of its two-dimensional visualization and flatus interference with the images. It is difficult to determine accurate positioning of a large mass when it is adhering closely to adjacent tissues. It is also difficult to determine the extent of tumor invasion and the relationship between the tumor and its surrounding tissues.
CT examination leads to misdiagnosis of pelvic tumors
Enhanced abdominal pelvic CT examination (of a huge teratoma protruding to the pelvic cavity and squeezing the uterus and bladder and displacing adjacent bowels) combined with the fact that teratomas frequently occur in the ovaries inevitably lead to the misdiagnosis that the tumor is located in pelvic cavity and derived from the ovaries. Careful examination of the CT scan can reveal clearly visible boundaries between a teratoma and the pelvic organs (e.g., ovary and uterus). An enhanced CT scan can show accurately the tumor's location, size, shape, extent, relationship with surrounding tissues, characteristics, and intratumor composition. The nature of the tumor, invasion, and involvement of important blood vessels can be assessed according to the degree and manner of enhancement. These imaging characteristics can reflect the pathologic characteristics of the tumor. However, histologically similar germ-cell tumors may have similar imaging characteristics although their positions are different. 13 Therefore, CT scans should be examined carefully for atypical tumor characteristics to prevent misdiagnosis.
Conclusions
A preperitoneal primary teratoma is rare. Detailed inquiry and comprehensive examination is very important to differentiate this kind of tumor from other related conditions.
Footnotes
Disclosure Statement
No competing financial conflicts exist.