
Abstract
Abstract
Introduction
Exploratory laparoscopy in conjunction with therapeutic management is of paramount importance. Laparoscopy currently becomes the first modality for any treatment at a single sitting, which has many advantages for physicians and patients. Herein is described a rare case of fibrothecoma in an 82-year-old woman who presented with abdominal distention, weight loss, and a large pelvic mass with an umbilical hernia.
Case
An 82-year-old Taiwanese woman presented to the Chang Gung Memorial Hospital with complaints of progressive abdominal distention along with significant weight loss; however, she denied having abdominal pain. Her relevant medical and surgical history included Parkinson's disease, hypertension, and total hip replacement 4 years earlier.
On physical examination, the abdomen was noted to be distended and there was a small palpable mass at the umbilicus. The patient had grade 2 pitting edema in her extremities. Her CA-125 was 125 U/mL.
A CT scan revealed a well-defined solid mass, located in the right ovary, suggestive of ovarian cancer, measuring 12.4×11.4×6.3 cm. Ascites, small cysts in both the liver and the pancreas, and an umbilical hernia were also reported (Figs. 1 and 2).

Computed tomography showing no ascites, small umbilical hernia, and no para-aortic lymph node enlargement.
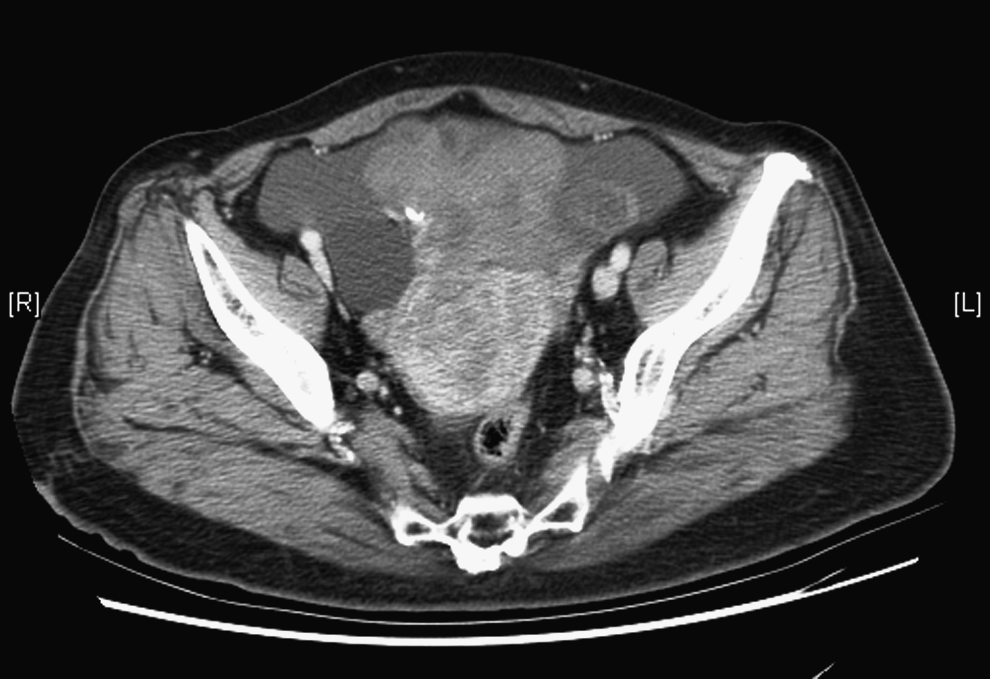
Computed tomography revealing a right ovarian cancer, small myoma, and no iliac lymph node enlargement.
Because of the age of the patient and her large pelvic mass complicated by the umbilical hernia, a single-sitting laparoscopic-assisted vaginal hysterectomy with bilateral salpingo-oophorectomy and hernioplasty was planned. The Lee–Huang portal was used, because primary trocar insertion was in the middle upper abdomen between the xiphoid process and the umbilicus, 5 and three other trocars were inserted for three-handed surgery.
During the exploratory laparoscopy, umbilical herniation was seen (Fig. 3). The omentum filled the umbilical hernia sac, but neither incarceration nor strangulation were noted. Reduction of the hernia content from the umbilical hernia sac measuring 2.5 cm in diameter (Fig. 4) was performed. Neither necrosis nor infarction was noted at the omentum. The right solid ovarian tumor measured 15 cm in diameter with an intact capsule and a smooth surface. The uterus, left ovary, and both Fallopian tubes were grossly normal. There were 100 cc of ascites. Laparoscopic-assisted vaginal hysterectomy with bilateral salpingo-oophorectomy was performed first. The ovarian mass, uterus, left ovary, and both Fallopian tubes were removed with vaginal morcellation, using a cold knife.
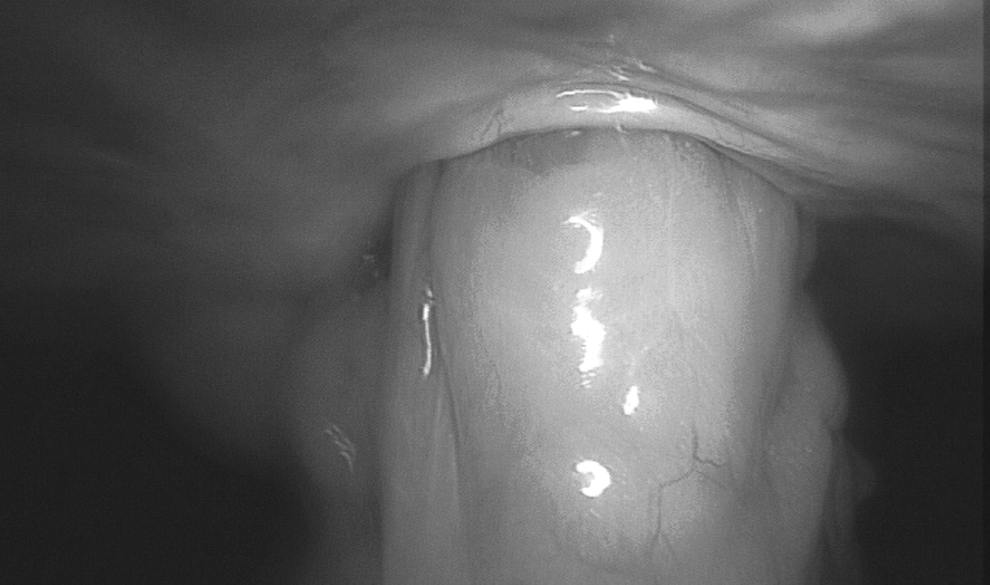
Laparoscopy findings of omentum occupying the hernia sac.

Laparoscopy finding of the diameter of the hernia sac.
Afterward, the Mayo hernia repair was performed. Excision of the hernia sac from the fascia rims was performed, and then the anterior and posterior fascia were repaired by primary closure of overlapping fascia using a continuous running suture with monofilament polypropylene nonabsorbable suture number 1/0 (Prolene; Ethicon, Somerville, NJ). The result can be seen in Figure 5.

Results of the suturing with nonabsorbable suture (Prolene).
Results
The patient had an uneventful recovery and was discharged on postoperative day 3.
Histologic examination of the section from the right ovarian tumor revealed a fibrothecoma.
Two years after the surgery, the patient was well and asymptomatic.
Discussion
Ovarian fibrothecomas are uncommon tumors that arise from gonadal stromal cells. These tumors can occur at any age, but the peak incidence is after menopause.1,3
The preoperative diagnosis of this neoplasm is difficult, because there are no characteristic symptoms and there are variable imaging features. In this patient, the symptoms (abdominal distention and weight loss) and the CT scan revealed malignancy of the ovarian tumor with ascites. Son et al. reported that 34% of women were misdiagnosed preoperatively, but that accurate magnetic resonance imaging may prevent excessive surgical intervention.1,2
Studies have found ascites in 31.9%–67% women during surgery. 2 These ascites are related to the increased levels of CA-125, in which the tumor itself forms a transudate. 2
Umbilical hernia in adults is an acquired hernia in almost 90% of cases, and it more commonly occurs in women than in men. 6 This hernia is associated with obesity, multigravida status, previous surgery, and high abdominal pressure (ascites, coughing, and straining).
In this patient, the abdominal distention happened because the ascites and large pelvic mass caused the high intra-abdominal pressure that leads to umbilical hernia, which she was also predisposed to by weakened fascial tissue at the umbilicus caused by ageing, multigravida status, and obesity.
The major complications of hernias are incarceration (in hernias <1.5 cm in diameter), strangulation, and evisceration.
Surgical management was recommended as treatment, after considering many factors such as the patient's age, expectation of slow healing, the removal of the large ovarian mass, ascites, and umbilical hernia repair.
Minimal invasive surgery was performed: In this case, the procedure was laparoscopic-assisted vaginal hysterectomy with bilateral salpingo-oophorectomy, and umbilical herniorrhaphy.
The authors of this article have been using the Lee–Huang portal for 15 years, and find it safe and practical, especially when dealing with large pelvic masses and adhesions in the umbilicus. The median incision through the linea alba prevents penetrative injury to major blood vessels. This provides a wider access to the abdominal cavity and increases the working distance, which supports a better visual angle. 7
Compared with the open technique, laparoscopic surgery for umbilical hernia provides reduced perioperative morbidity, less postoperative drainage and pain, reduced recovery time, and low recurrence rate (7.7% versus 11%). Moreover, recurrent umbilical hernias of any size benefit from the laparoscopic technique. 8 Obese patients would have many advantages from this laparoscopic repair, with its lower infection and recurrence rate. In this patient, laparoscopic umbilical hernia repair was performed because this approach allowed wider fascial closure, easier adhesiolysis, and retraction of the hernia to the abdominal cavity under direct vision, and it eliminated the need for anterior tissue dissection.
A recent Cochrane review calculated a pooled infection rate of 10.1% for hernia repair with mesh. This can lead to infection of the prosthesis, and sometimes it is necessary to perform mesh removal.9,10
Conclusions
In conclusion, laparoscopy is a multifunction procedure with several advantages and minimal side-effects, especially for high-risk patients, and the Lee–Huang portal is very important for the laparoscopic approach.
Disclosure Statement
No competing financial interests exist.