
Abstract
Abstract
Introduction
Case
A 32-year-old woman was followed-up in a gynecology department with an initial presentation after an incidental finding of a 5-cm, predominantly solid mass that noted on an ultrasound scan (US) that was taken during a spontaneous first-trimester miscarriage. This patient had a history of an emergency lower-segment caesarean section in the same hospital unit 1 year prior to this miscarriage. At that time, it was documented that she had normal ovaries. There was no other significant medical or surgical history. However, she did report subsequently that she had antecedent chronic gynecologic symptoms of intermittent pelvic pain and deep dyspareunia.
A follow-up pelvic transvaginal US scan showed no change in the heterogeneous mass, which appeared to be arising from, or abutting, the posterior wall of the uterus near the cervix, which was more characteristic of a fibroid growth than a cyst. The right ovary was not visualized. Standard serum tumor markers were measured, including CA-125, and germ-cell tumor markers human chorionic gondadotropin (hCG), α-fetoprotein were all within normal range. Magnetic resonance imaging (MRI) was performed, but, initially, was reported as only showing a hemorrhagic ovarian cyst (Fig. 1).
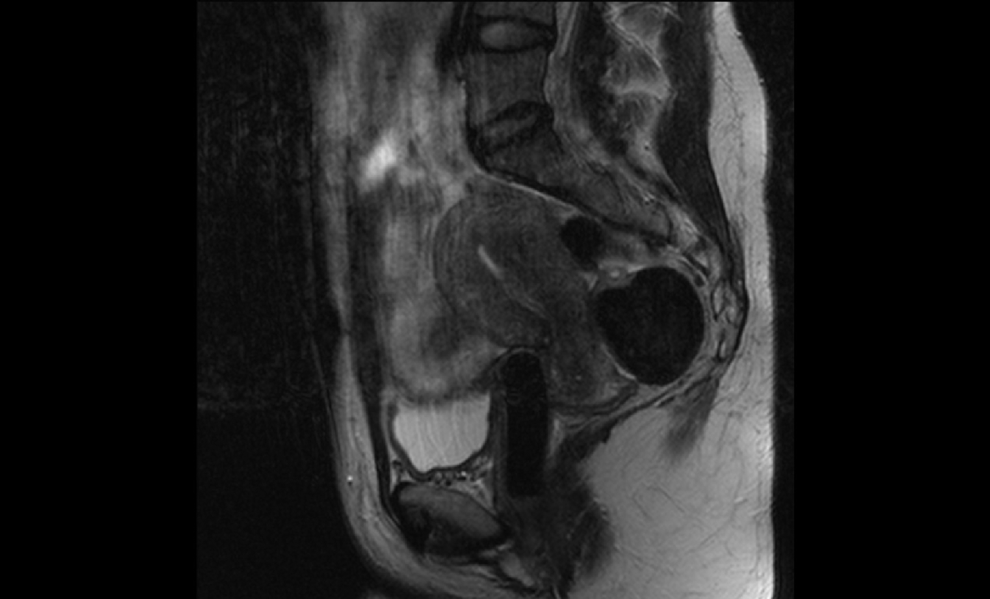
Magnetic resonance imaging sagittal T2 weighted sequence: 5-cm low-signal mass in the pouch of Douglas, with tiny cysts at the superior aspect of the mass.
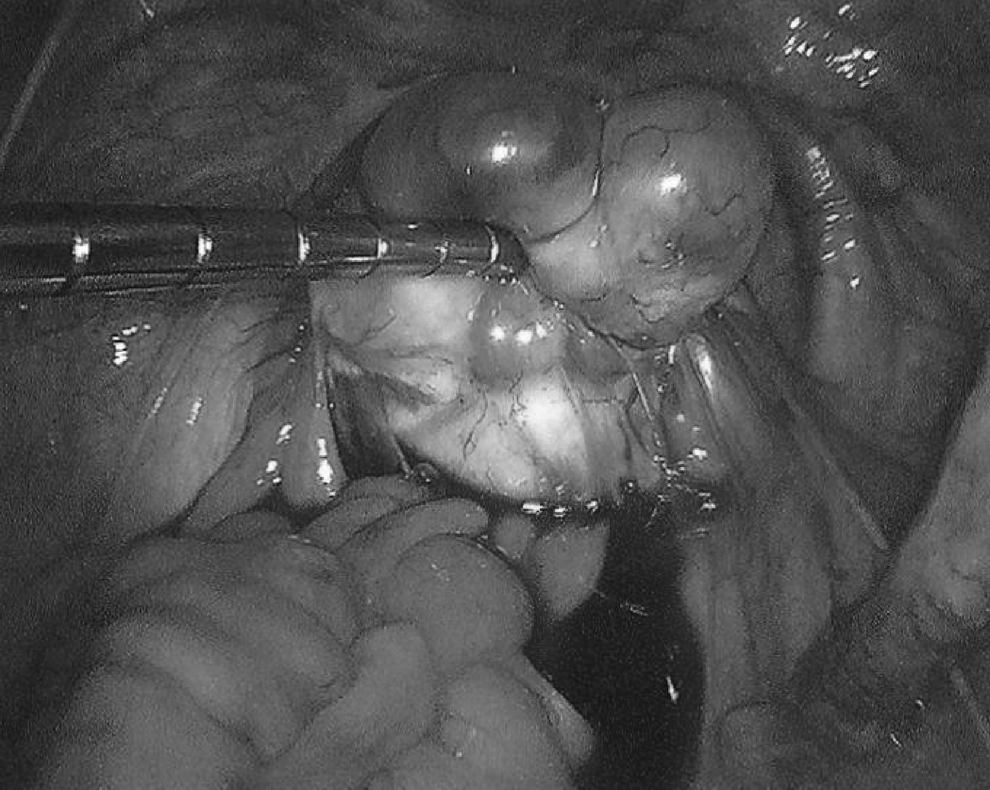
A diagnostic laparoscopy showed that this patient had an enlarged, globular left ovary containing a hemorrhagic cyst, with a much smaller, normal-looking right ovary. However, there was also a 5-cm solid mass within the recto-uterine Pouch of Douglas, initially raising suspicions of a “parasitic” fibroid growth (Fig. 2). The mass abutted the lower part of the right utero-sacral ligament. Neither of the adnexal structures or the uterine corpus or cervix uteri was visibly connected to the solid mass. A laparoscopic left ovarian cystectomy was performed, with subsequent histopathology confirming a functional corpus luteal cyst. Radiologists reviewed the initial MRI images afterward and confirmed that they were consistent with the presence of a solid lesion in the Pouch of Douglas, suggestive of a fibroid growth, close to the cervix uteri (Fig. 1). The rest of her pelvis and abdomen was structurally normal.

Initial laparoscopy showing bilateral normal ovaries along with an ectopic ovarian leiomyoma in the recto-uterine pouch of Douglas (without visible cystic areas).
This patient was followed-up and managed conservatively but continued to be symptomatic with pelvic pain. A second laparoscopy was performed, 10 months after the first procedure. Both of her ovaries appeared normal, with the 5-cm solid cul de sac mass still present, but with cystic-looking structures now arising from the solid areas (Fig. 3). It was confirmed to be separate from the broad ligament, both adnexal structures (Fallopian tubes and ovaries) and the uterine corpus and cervix uteri. Instead, the mass was attached to the mesentery of her rectum and peritoneum in the Pouch of Douglas, adjacent and medial to the lower end of the right utero-sacral ligament. The mass was mobilized and excised completely, without complications, using laparoscopic ultrasonic shears and scissors, with retrieval from the abdominal cavity utilizing a 12-mm laparoscopic port.
Second laparoscopy showing cystic areas on surface of the ovarian leiomyoma.
Results
The patient made an uneventful recovery from the abovementioned procedure. Subsequent histology, surprisingly, reported fragments of normal ovarian tissue with functional cysts (Fig. 4) as well as fragments of a collagenous leiomyoma (Fig. 5). Overall, this was consistent with an ectopic ovarian leiomyoma (despite no physical connection between the solid structure and the ovaries or uterus). The patient was followed up in the gynecology outpatient department subsequently, and she reported no further symptoms of pelvic pain following this excision.

Histologic image of the ectopic ovary showing the presence of normal ovarian tissue, including a functional cystic area.
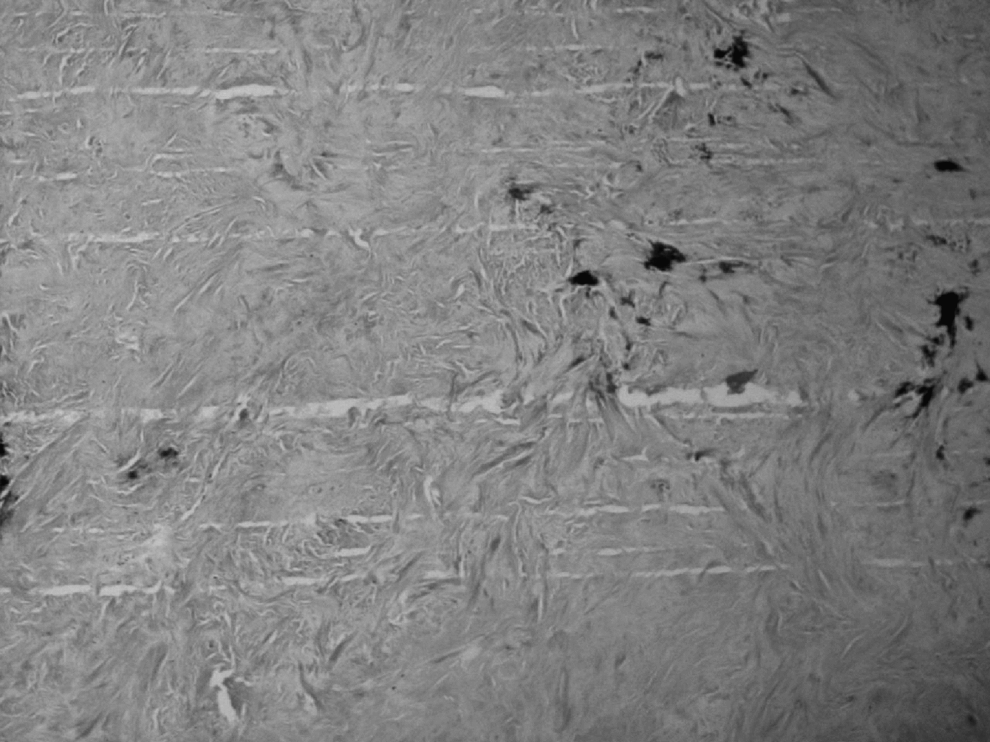
Histologic image of the ectopic ovary showing collagenous tissue suggestive of a leiomyoma.
Discussion
There has been debate regarding the definition and classification of ectopic ovary. 2 The condition has also been described as supernumerary, accessory. or auto-amputated ovary in different case reports. Winkle first reported a case of an ectopic ovary in 1890. Wharton described 2 cases of supernumerary and accessory ovary in 1959 3 and attempted classification of this entity. Accessory ovaries were described as the presence of an extra/additional ovary when the accessory ovary was present in close proximity to one of the normal ovaries, with some connections to it. A supernumerary ovary is present elsewhere, away from the normal ovaries and with no direct connections with them or with the broad ligament and uterus. A supernumerary ovary and usually present along the path of embryologic migration of the ovarian primordium, most commonly in the omentum. There have been ∼40 reported cases of accessory or supernumerary ovary, since Wharton's initial description of this condition.
The other descriptive terms reported in the literature are ectopic ovary, auto-amputated ovary and ovarian implant. Ectopic ovary can be defined as an ovary present in an abnormal location, and it could be either replacing one of the normal ovaries or present in addition to both the normal ovaries. Lachman and Berman. 2 suggested replacing the terms supernumerary and accessory with ectopic because the first two terms were confusing and did not explain all types of abnormally placed ovaries. Approximately 50% of these cases of additional ovarian tissue were reported as being acquired in origin, secondary to inflammation or surgery, and these have been described as ovarian implants. Therefore, ectopic ovary could be subclassified as true ectopic ovary, because of abnormal embryologic migration (irrespective of its location), post-surgical implant, and post-inflammatory implant. True ectopic ovary can be sub-classified as an abnormally located ovary, replacing the normal ovary on one side (i.e., a normal complement of two ovaries overall) or an extra ovary in addition to the two normally located ovaries. The presence of an abnormally located ovary is known to be associated with other congenital malformations, mainly pelvic and renal, in up to 36% of cases. 1
Different types of tumors have been reported in ectopic ovarian tissue such as cystadenomas, 4 benign teratomas,5,6 Brenner's tumors, 7 and fibromas with Meig's syndrome. 8 There have also been cases reported in which an ovary with a benign teratoma had auto-amputated and transplanted in an indirect inguinal hernia 6 and in the recto-uterine cul-de-sac, rectosigmoid colon mucosa 9 secondary to torsion. The ovarian tissue present in these locations with the teratomas were either each the only ovary from one of the normal locations or an accessory/supernumerary ovary.
Ovarian leiomyoma is a very rare benign tumor of the ovary arising from the smooth-muscle cells in the ovarian stroma/cortex, and diagnosis is often mistaken preoperatively as a fibroma, thecoma, uterine myoma, and or other benign tumor. 10
This is the first reported case of a true ectopic ovarian leiomyoma to the current authors' knowledge. The extra ovary was truly ectopic, as it was laparoscopically confirmed to be separate from both adnexal structures/ovaries, the broad ligament, and the corpus uteri/cervix uteri. The origin of this mass was possibly acquired secondary to some torsion or inflammatory process, which was explained by this patient's history of pelvic pain, although her only previous surgery was an emergency lower-segment caesarean section and both ovaries had been recorded as being normal at that time. However, it would not be normal practice to assess the pouch of Douglas during this procedure.
Conclusions
This case confirms that preoperative and prehistologic diagnosis of an ectopic ovary can be extremely difficult because this phenomenon is so rare. Consequently, it would not be considered as a potential diagnosis in most patients with chronic pelvic pain symptoms. Various forms of available imaging, such as pelvic US or MRI can provide detailed information regarding pelvic masses. However, the rarity of this particular phenomenon makes it difficult to predict the presence and the exact nature of ectopic ovarian tissue before histologic examination. Nevertheless, this case is an example of successful management of the condition using minimally invasive surgery that produced good symptomatic relief.
Footnotes
Disclosure Statement
The authors report no conflicts of interest.