Background: Understanding of ovarian pregnancy is poor, because of the rarity of the condition. The exact etiology is unknown, preoperative diagnosis is a challenge, and clinical presentation is highly variable. Generally, ovarian pregnancies rupture later than tubal gestation, and there are reports of ovarian pregnancies continuing right up to the third trimester. Case: A case of very early rupture of an ovarian pregnancy on day 28 of the cycle, along with a review of the literature to determine usual gestation at the time of rupture of spontaneously conceived ovarian pregnancies, is presented. Results: Wedge resection of the left ovary with complete removal of ectopic gestation was performed, and postoperative recovery was uneventful. Histopathologic examination confirmed an ovarian pregnancy. Conclusions: Data collected in this report suggest that nearly three-fourths of spontaneously conceived ovarian pregnancies rupture at or after 8 weeks of gestation, which is higher than in previous reports. Rupture of ovarian pregnancy on day 28 of the cycle is very unusual, and a possible cause is discussed briefly. (J GYNECOL SURG 29:245)
Introduction
Since its first description by St. Maurice in 1685, and diagnostic criteria provided by Spielberg1 more than a century ago, nothing major has been added to the literature of primary ovarian pregnancy, in particular regarding the natural course. The list of risk factors is vague, and the exact etiology is unknown. Preoperative diagnosis is a challenge, and is likely to be made on the operating table or during histopathologic examination. This is not surprising, given the rarity of the disease, with a reported incidence of 1 in 7000 to 1 in 60,000 deliveries.2 However, the management of primary ovarian pregnancy has evolved (albeit slowly), largely because of improvements in ultrasound technology and minimally invasive surgery. Ovarian pregnancies tend to rupture late because of a thick ovarian capsule, and there have been reports of ovarian pregnancies continuing right up to third trimester. A case of unusual early rupture of ovarian pregnancy at day 28 of the cycle, along with a review of case reports of ruptured ovarian pregnancies published in English literature over last 20 years, to determine when an ovarian pregnancy usually does rupture, is presented.
Case
A 25-year-old para 2 reported on the day of her expected menstruation with acute pain of sudden onset in the lower abdomen, of 4–6 hours' duration. There were no urinary or gastrointestinal complaints. She had experienced a similar episode 1 week earlier but her pain was relieved with medication. She reported regular menstrual cycles of 28 days' duration, and denied usage of any hormonal contraceptive method. Her obstetric history was notable for two normal deliveries. She had moderate pallor and tachycardia, and her blood pressure was 100/60 mm Hg. Her abdomen was soft, and there were no signs of peritoneal irritation. Bimanual examination revealed a normal-sized uterus with cervical motion tenderness, and a tender ill- defined mass in the left adnexal region. Her hemoglobin was 6.8 gm% and hematocrit was 27%. Transabdominal ultrasound revealed an empty uterus, complex left adnexal mass of 4×5 cm, and moderate free fluid in the peritoneal cavity. No ectopic gestational sac or fetal node was visualized. Urinary human chorionic gonadotropin (HCG) was positive, and serum sample was collected for β HCG estimation. Laparotomy was performed in view of strong suspicion of ruptured tubal ectopic pregnancy. There was 500 mL of blood with clots in pouch of Douglas peritoneal cavity. Uterus, Fallopian tubes, and right ovary appeared grossly healthy. Left ovary was enlarged to 5×5 cm with a rent in the lateral pole, and a fleshy mass was seen projecting outside from that rent (Fig. 1). Wedge resection of left ovary with complete removal of ectopic gestation was performed. Histopathologic examination confirmed ovarian pregnancy (Figs. 2 and 3), therefore fulfilling all Spielberg's criteria. Preoperative serum β HCG value of 228 milli-international units (mIU/)mL was obtained, which showed a steady decline, with normalization within a few days following surgery. The patient received 2 U of blood intraoperatively, and her postoperative (day 1) hemoglobin was 9 gm%.
Ruptured left ovarian pregnancy.
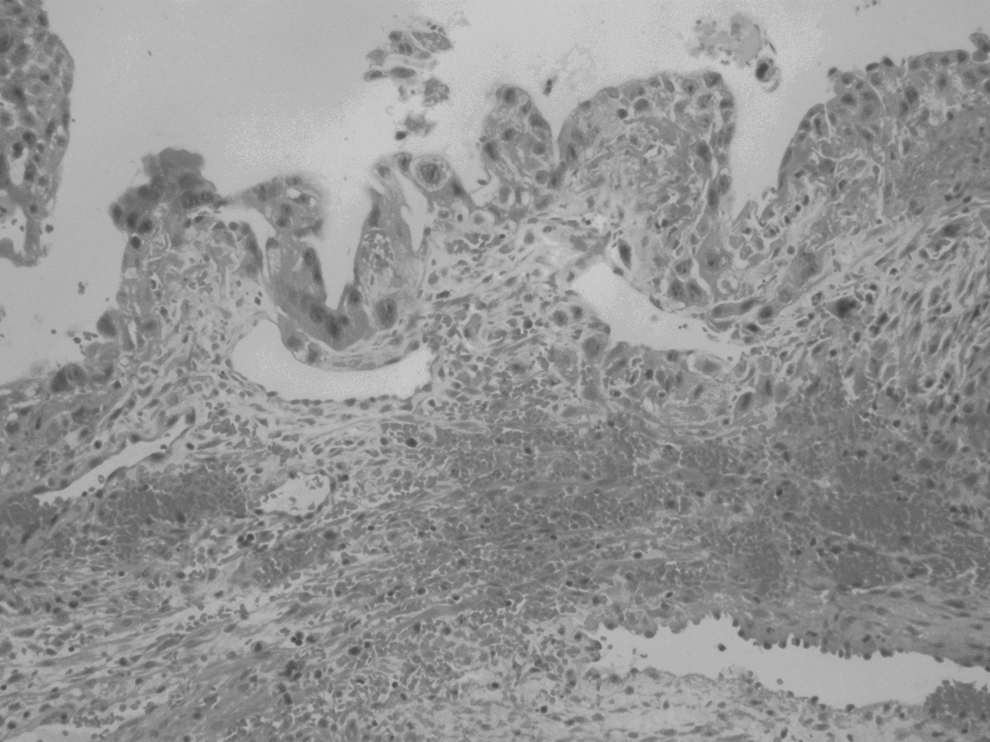
Hematoxylin and eosin. Cystic lesion with wall composed of ovarian stroma and lined by trophoblastic cells.
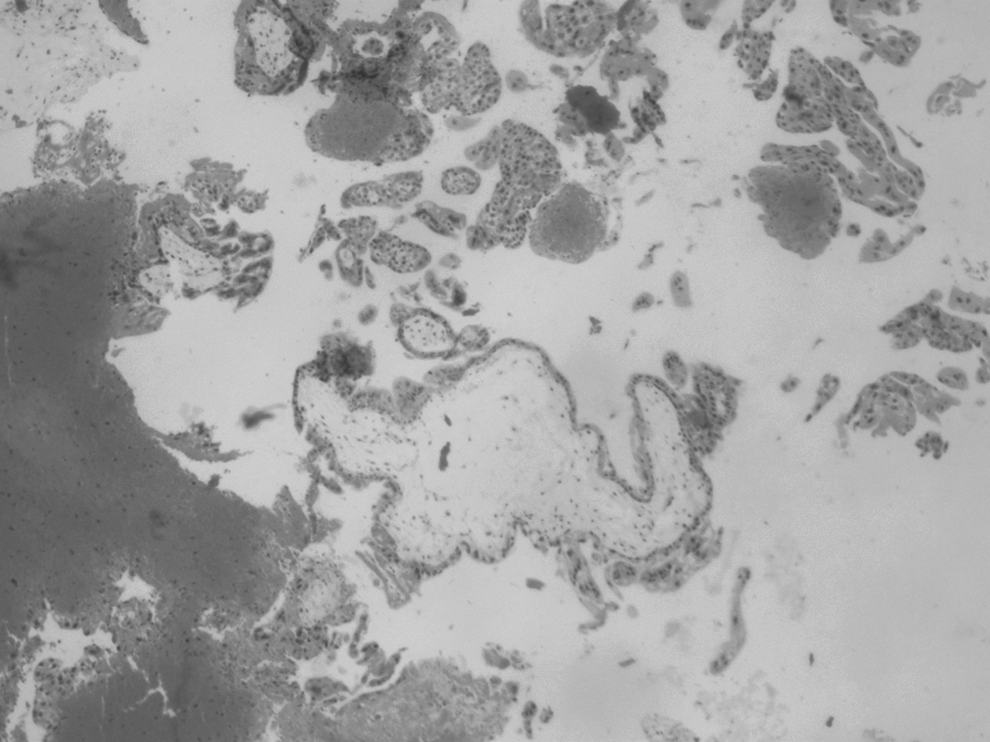
Hematoxylin and eosin. Presence of chorionic villi within the parenchyma of the ovary.
Results
The postoperative period was uneventful, and this patient was discharged on day 5 afterward.
Discussion
The exact etiology of ovarian pregnancy is not known; however, it has been postulated that it results, either from intrafollicular fertilization or by retrotubal flow of the embryo with subsequent ovarian implantation.3 The list of risk factors is vague; however, there is a general agreement that the classic risk factors of ectopic pregnancy, such as pelvic inflammatory disease, tubal surgery, previous ectopic pregnancy, and infertility, are usually absent in women with primary ovarian pregnancy. An association between intrauterine device use and ovarian pregnancy has been suggested.4 The clinical presentation of primary ovarian pregnancy is highly variable, with abdominal pain and vaginal bleeding being the most common presenting complaints. However, 50% of ovarian pregnancies following ovarian hyperstimulation are diagnosed at an asymptomatic stage.3 Clinical presentation of primary ovarian pregnancy does not differ from that of other ectopic pregnancies; there are, however, some differentiating features. The symptom of pain is less prominent with ovarian pregnancy than with tubal gestation, as the former lacks the neurogenic element of pain associated with stretching, that occurs with tubal ectopic gestation.5 Ovarian pregnancies tend to rupture late, largely because of ovarian capsule having greater stretch ability than the Fallopian tube. A PubMed database search was performed, for reports of ruptured ovarian pregnancies published in the English literature from 1990 to 2012, using key words ovarian pregnancy, ruptured ovarian pregnancy and primary ovarian pregnancy. For the purpose of reviewing, only reports of spontaneously conceived ovarian pregnancies, fulfilling all the Spielberg's criteria, and with reasonable certainty of gestational age, were included. A total of 12 case reports (13 cases) fulfilled these criteria,6–16 details of which are given in Table 1. Three fourths of the cases (10) ruptured at 8 week or later, and in nearly 50% of cases (6 cases) rupture occurred at or after 9 weeks of gestation, which is a slightly higher percentage and longer gestation than those quoted by Sandberg et al.17 Early rupture on day 28 of the cycle is an unusual presentation. Estimation of gestational age, based on the subject's last menstrual period, was fairly accurate in this case, as she had experienced regular menstrual cycles of 28 days' duration earlier, with her last menstruation being normal, and she denied having used any kind of hormonal contraception previously. Moreover, β HCG value of 228 mIU/mL seems to support an early gestation, even though in ovarian pregnancy β HCG values tends to be low and rise slowly. Histopathologically, ovarian pregnancy has been categorized into intrafollicular and extrafollicular types. Extrafollicular ovarian pregnancy is further subdivided into juxtafollicular, interstitial, cortical, and superficial types, based on anatomic location within the ovary.18
Review of the 13 Cases of Ruptured Ovarian Pregnancies, Following Spontaneous Conception, Reported in the English Literature Between 1990 and 2012, Listing the Gestation at the Time of Rupture
CRL, crown rump length; hCG, human chorionic gonadotropin; mIU, milli-international units; MTX, methotrexate; MSD, mean sac diameter.
Conclusions
Many people have criticized this classification system as being an academic exercise only. However, anatomic location of the gestational sac seems to offer a plausible explanation for very early rupture of ovarian pregnancy in this case. In an extrafollicular superficial ovarian pregnancy, there is a theoretical probability of early trophoblastic invasion, and consequent rupture of the otherwise thick ovarian capsule.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
1.
SpielbergO. Zur kasuistik der ovarialschwangerschaft. Arch Gynaekol, 1878; 13:73.
2.
GaudoinMR, CoulterKL, RobinsAMet al.Is the incidence of ovarian pregnancy increasing?Eur J Obstet Gynecol Reprod Biol, 1996; 70:141.
3.
MarcusSF, BrinsdenPR. Primary ovarian pregnancy after in vitro fertilization and embryo transfer: Report of seven cases. Fertil Steril, 1993; 60:167.
4.
JosephRJ, IrvineLM. Ovarian ectopic pregnancy: Aetiology, diagnosis and challenges in surgical management. J Obstet Gynecol, 2012; 32:472.
5.
EskandarO. Conservative laparoscopic management of a case of ruptured ovarian ectopic pregnancy by using a harmonic scalpel. J Obstet Gynecol, 2010; 30:67.
6.
SidekS, LaiSF, Lim-TanSK. Primary ovarian pregnancy: Current diagnosis and management. Singapore Med J, 1994; 35:71.
7.
ErcalT, CinarO, MumcuA, LacinS, OzerE. Ovarian pregnancy: Relationship to an intrauterine device. Aust NZ J Obstet Gynaecol, 1997; 37:362.
8.
MarretH, HamamahS, AlonsoAM, PierreF. Case report and review of literature: Primary twin ovarian pregnancy. Hum Reprod, 1997; 12:1813.
9.
VarrasM, PolizosD, KalamaraCh, AntypaE, TsikiniA, TsouroulasM, AntoniouS, PaissiosP. Primary ruptured ovarian pregnancy in a spontaneous conception cycle: a case report and review of literature. Clin Exp Obstet Gynecol, 2002; 29:143.
BoronowR, Mc ElinTW, WestRH. Ovarian pregnancy. Report of four cases and a thirteen year survey of English literature. Am J Obstet Gynecol, 1965; 143:55.