
Abstract
Abstract
Introduction
Case
A 55-year-old woman, para 8, was admitted to a department of obstetrics and gynecology at a health care facility on November 17, 2011 with a complaint of polymenorrhagia of 2 months' duration. There was no associated history of abdominal pain, distention, or dysmenorrhea. The patient's previous menstrual cycles had been regular, with average flow lasting 3–5 days. She had never used any hormonal contraception. Abdominal examination showed no abnormality. Gynecologic examination revealed a normal size uterus. A mobile mass of 7×7 cm was palpable through the right fornix, in close proximity to the uterus. Ultrasonography also showed a solid pelvic mass measuring 9.1×6.3 cm, with small cystic areas suggestive of a right ovarian tumor or subserous fibroid. Serum CA-125 level was 6.9 U/mL.
The patient subsequently underwent laparotomy on November 21, 2011. Her abdomen was opened through an infraumbilical midline vertical incision. After the skin and rectus sheath were incised, the rectus abdominal muscle was separated. Thereafter, the parietal peritoneum could not be lifted up as a thin fold. Instead, a soft-tissue mass of 6×6 cm was palpable in the peritoneum. This mass mimicked adhered bowel loops. The abdominal incision was extended upwards, and careful dissection revealed a free fold of peritoneum beyond the upper limit of the mass. The peritoneum was opened and the mass was then noted to be a soft-tissue mass in the peritoneum (Fig. 1). The mass was soft and fleshy. The undersurface was smooth and free from all intra-abdominal organs. It was removed intact, with overlying peritoneum. The intestines and omentum showed no abnormality. The uterus was smooth and mildly enlarged. Bilateral adnexae were normal. Panhysterectomy was performed. The open specimen of peritoneal mass was suggestive of hyaline changes. The specimen of the uterus showed myohyperplasia.
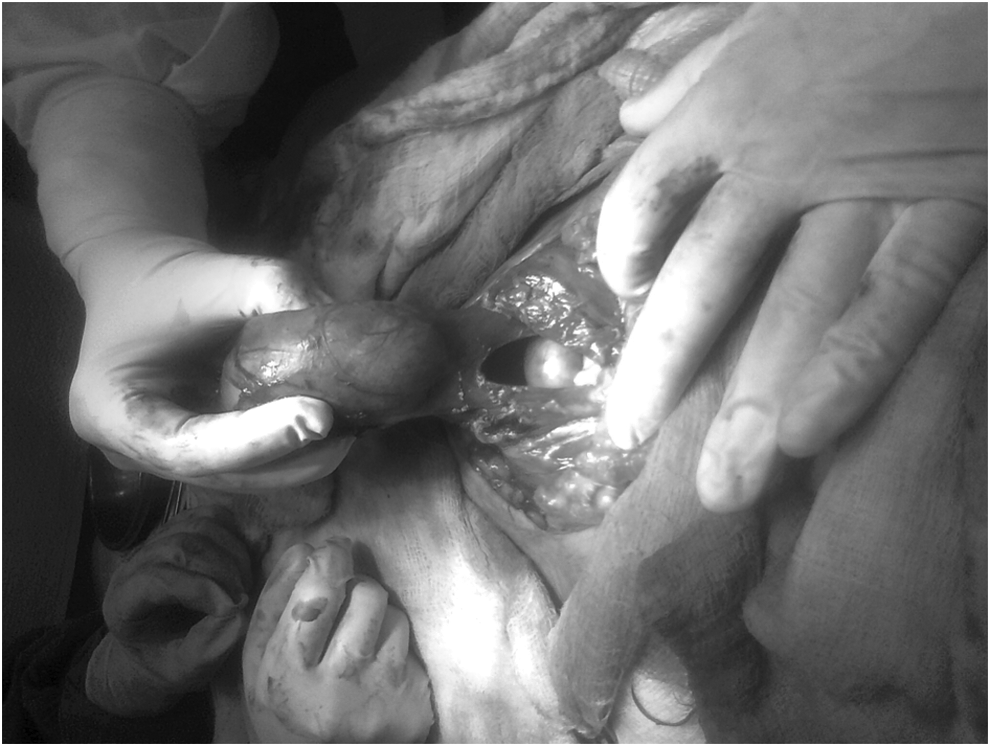
Peritoneal leiyomyoma seen on opening the peritoneum.
Results
Histopathology of the peritoneal mass confirmed a serosal leiomyoma with foci of hydropic degeneration. Histopathology of the uterus showed nonsecretory endometrium, papillary endocervicitis, and hypertrophied squamous epithelium. The right ovary showed a corpus luteal cyst. The rest of the adnexa was essentially normal histologically. The patient was discharged in satisfactory condition on the eigth postoperative day.
Discussion
Extrauterine leiomyomas at unusual sites are described as DPL, parasitic leiomyomata, intravenous leiomyomatosis, retroperitoneal leiomyomata, and benign metastasizing leiomyoma. 1
Disseminated peritoneal leiomyomatosis is a rare condition characterized by nodular proliferation of histologically benign smooth muscle throughout omental and peritoneal surfaces. It is usually found in females of reproductive age, but cases have been described in both the postmenopausal and fetal periods. It is associated with the altered hormonal environment of pregnancy, steroid-secreting ovarian tumors, and oral contraceptive use. Its hormonal responsiveness is suggested by the presence of estrogen and progesterone receptors. Most DPL cases behave in a clinically benign fashion, and in some instances, the lesions may partially or completely regress. Alternatively, DPL may progress, recur, or undergo malignant transformation. In light of the benign histology, association with altered steroid hormone levels, and generally benign clinical course, DPL has been interpreted to be a metaplastic proliferation derived from undifferentiated subperitoneal mesenchymal cells. 2
On rare occasions, pedunculated subserous leiomyoma detach from their primary site and implant elsewhere in the pelvis, the process involving a combination of inflammation and infarction. The tumor then begins to derive its blood supply from the new site of attachment. Sometimes, it may preserve its initial attachment to the uterus. Okoro et al. 3 reported a rare case of a large degenerated parasitic leiomyoma in the peritoneal cavity deriving its blood supply from the omentum, and attached to a normal-looking uterus by a narrow avascular stalk.
Although several instances of disseminated peritoneal and parasitic leiomyoma have been described in the literature, an isolated peritoneal leiomyoma with an essentially normal uterus has been rarely described. One such tumor was reported by Sang et al. 4 in a 51-year-old patient. The solid tumor of 18 cm diameter in the peritoneal wall was histologically diagnosed as a benign leiomyoma. The tumor encountered in the patient presented here was similar, because the uterus was normal and no attachment to the uterus was identified. Such isolated tumors in the peritoneum may be derived from smooth-muscle cells or mesenchymal cells in the peritoneum.
Among other extrauterine leiomyomas, intravenous leiomyomatosis 5 is characterized by nodular masses of histologically benign smooth-muscle cells growing within venous channels. Grossly, it is a growth in the myometrium with wormlike extensions within the veins of the broad ligament or the uterine veins. Extensions up to the vena cava have been reported in <10% of cases.
Conclusions
Benign metastasizing leiomyoma 5 is a rare condition in which metastatic smooth muscle tumor deposits are seen in the lungs, lymph nodes, and abdomen, and have apparently been derived from benign uterine leiomyomas. Hormone dependence of these tumors is suggested by the finding of estrogen and progesterone receptors in the tumors.
Retroperitoneal leiomyomas are mostly (73%) located in the pelvis. They present as retroperitoneal masses, leading to high suspicion of malignancy. Poliquin 6 and coworkers found an association between retroperitoneal leiomyomas and uterine leiomyomas or a history of hysterectomy for uterine leiomyomata in 40% of their series of 37 cases. Zaitoon et al. 7 suggested the parasitic theory, whereas Kho and Nezhat 8 proposed an “iatrogenic” origin for such growths. They found that more parasitic myomas may be created after morcellation techniques.
Leiomyomas of deep soft tissue are diagnosed on the basis of absence of nuclear atypia, necrosis, and minimal mitotic activity. 9 They are seen in both males and females. Although they resemble uterine leiomyoma, they are always distinct from the uterus.
Footnotes
Disclosure Statement
There are no commercial associations that might create a conflict of interest among any of the authors. There are no conflicts of interest, whether actual on potential, to be disclosed.