
Abstract
Abstract
Introduction
L
This article reports a rare case of lipoleiomyoma of the cervix that was diagnosed in a 40-year-old premenopausal woman, who received an exploratory laparotomy with a preoperative diagnosis of a solid adnexal mass suggesting an ovarian malignancy. Related articles are also reviewed. This case is reported because these growths are rare, and this case had a rare presentation.
Case
A 40-year-old, gravida 3, para 3, premenopausal woman presented to the current authors' gynecology department with pain in her abdomen and dyspepsia for 45 days. The patient's history revealed menarche at age 15, regular menstruation of 3–4 days duration, and an average flow with dysmenorrhea at 30-day intervals. She had given birth 3 times, with her last delivery occurring 16 years prior to presentation. Her family history was not significant. There was no history of diabetes, hyperlipidemia, hypertension, or other metabolic and endocrine disorders.
A general physical examination did not detect any abnormalities. An abdomenal examination indicated the presence of mass ≤16–18 weeks size. A vaginal examination showed that her cervix pushed upward and anteriorly, and a large mass ∼10 cm, immobile, variable in consistency, was felt below her pubic symphysis. When it was palpated, this mass did not seem to be separated from uterus. The size of uterus was not discernable.
The results of routine biochemical and hematologic investigations were within normal limits. Ultrasonography (USG) of the patient's pelvic area showed a normal-size (84×60×37 mm) anteverted uterus with a regular and smooth margin. There was evidence of a very large, complex echoic lesion in the pouch of Douglas and bilateral adenexa causing anterior displacement of the uterus. This mass measured >140×91 mm. The overies could not be visualized separately. No free fluid was seen in the pouch of Douglas. Thus, this USG scan indicated the presence of large pelvic space-occupying lesion (SOL). A contrast-enhanced computed tomography (CECT) scan of the whole abdomen showed a large, well-defined, lobulated, heterogeneously hypodense, abdominopelvic mass lesion measuring ∼203×166×101 mm, with an enhanced solid component and multiple septa of variable thicknesses. Both ovaries were not visualized separately. The CECT scan results were suggestive of a mitotic neoplasm with an etiology of ovarian origin (Fig. 1). Although the current authors emphasized the diagnostic value of magnetic resonance imaging (MRI), the patient refused to undergo this scanning because of the cost involved.

Computed tomography scan shows a huge abdominopelvic mass with heterogenous attenuation.
This patient was admitted with a preliminary diagnosis of an ovarian malignancy and she was scheduled for a total abdomen hysterectomy with a bilateral salpingo-oophorectomy and an omenectomy. During this operation, the neoplasm was found to be large subserosal cervical fibroid growth arising from the patient's abdomen, involving her uterus and cervix. Both ovaries were found to be healthy during the operation and thus were retained in situ. A specimen of the neoplasm sent for histopathologic examination.
On gross appearance, the uterus and cervix measured 8×6×4 cm, and a large, encapsulated, well-circumscribed, solid, ovoid, subserosal mass measured 20×15×10 cm was attached to the posterior aspect of cervix (Fig. 2). On serial cut sections, the capsulated mass showed pale yellow-to–gray-brownish areas and was soft to firm in consistency. No areas of necrosis and hemorrhage were seen. The uterus and cervix were macroscopically normal.

The uterus and cervix with a huge capsulated oval subserosal mass measuring 20×15×10 cm.
Paraffin-embedded sections were prepared from the neoplasm and were stained with hematoxylin and eosin. Microscopically, the sections from the neoplasm showed a mixture of bland, spindle-shaped smooth-muscle cells in a whorled pattern with mature adipocytes (Figs. 3 and 4). No cytologic atypia (in smooth-muscle cells or adipocytes), necrosis, or calcification were seen. Sections from the endometrium and cervix were unremarkable. With these histopathologic findings, the neoplasm was diagnosed as a benign lipoleiomyoma of the uterus.
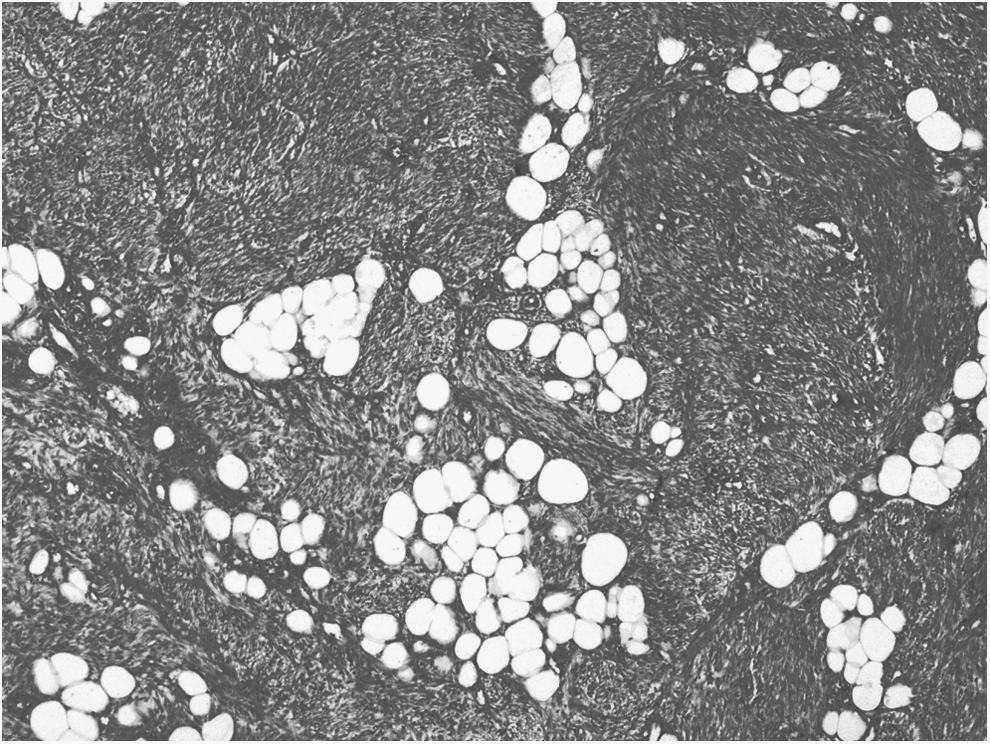
Histopathologic section showing the tumor composed of spindle-shaped smooth muscle cells in a whorled pattern with mature adipocytes (H&E stain×40).

Histopathologic section showing the tumor composed of smooth-muscle cells and adipocytes without atypia (H&E stain×100).
Discussion
Lipomatous uterine tumors are uncommon benign neoplasms that can generally be subdivided into two types: pure or mixed lipomas. The latter category consists of lipoleiomyomas, angiomyolipomas, and/or fibrolipomas. A third group of neoplasms has been proposed: malignant liposarcomas.2,3 Primary liposarcomas of the uterus are extremely rare and are most likely to arise from malignant transformation of lipoleiomyomas. 4
Lipoleiomyomas are rare benign neoplasms that are predominantly located in the uteri. The reported incidence of these neoplasms varies from 0.03% to 0.2%. 1 They usually occur in the uterine corpus, predominantly intramurally, especially within the posterior wall; however, they may be submucosal and subserosal as in the current case.5–8 Lipoleiomyomas may be found in the cervix, as in the current case, and extrauterine locations such as the broad ligament of the uterus, ovary, and peritoneum.7–11 This entity has been reported to range from 3 mm to 32 cm in diameter (with an average size, between 5 and 10 cm). 2 Uterine lipoleiomyomas most frequently occur in perimenopausal and postmenopausal women between ages 45 and 70, but the current patient was premenopausal. Contrary to uterine myomas, which are usually found in women of reproductive age, and which regress after menopause, lipoleiomyomas are more frequently found in older patients. 12 Concomitant uterine leiomyomas are commonly found, although this is not present in all patients, including the current case. 13
The clinical features are similar to those caused by a leiomyoma, such as a palpable pelvic mass, pelvic pain and discomfort, urine frequency, constipation, vaginal bleeding, etc. These symptoms are related to the size and location of the lesion. Most patients are asymptomatic. Some research showed an association of lipoleiomyomas with hyperlipidemia, diabetes, and hypothyroidism.14,15 In the current case, the patient did not have any metabolic and endocrine disorders.
Histologically, lipoleiomyomas consist of spindle-shaped smooth-muscle cells, in a whorled pattern admixed with varying amounts of mature adipose tissue, which do not show cytological atypia. The nuclei of the smooth-muscle cells are elongated and have finely dispersed chromatin and small nucleoli. The adipose component is entirely mature, without any lipoblasts, and may be regularly positioned within the tumor or may have a focal location.16–19 The amount of adipose components varies from 5% to 95% of the tumor mass. 7 The histologic differential diagnosis of similar uterine tumors with adipose tissue and spindle cells include: spindle cell lipomas; angiolipomas; angiomyolipomas; myelolipomas; atypical lipomas, and well-differentiated liposarcomas. 7 Rarely, cartilagenous differentiation or anomalous arterial blood vessels, resembling those seen in renal angiomyolipomas are noted. 13 A case of plexiform lipoleiomyoma with amyloid deposition has been reported in the literature. 20 Some researchers have described widespread infiltration of lipoleiomyomas by numerous small mature lymphocytes.21,22
Because fat tissue is not native to the myometrium, various theories have been proposed for the histogenesis of these tumors. A immunohistochemical study suggested that fatty metamorphosis of smooth-muscle cells of a leiomyoma or transformation of a totipotent mesenchymal cell into adipocytes is the most likely etiologic factor in the formation of adipose tissue, rather than fatty degeneration.7,13,16,23 Immunohistochemical analysis has shown an expression of S 100 in lipocytes, whereas leiomyomatous cells express smooth-muscle actin. 16 It has been suggested that metabolic changes occurring in postmenopausal women are a likely cause for the development of adipose tissue metamorphosis in lipoleiomyomas. 14
As seen on USG, the lesion is echogenic and is usually partially encased by a hypoechoic rim. The hypoechic rim is thought to represent a layer of myometrium surrounding the fatty component. However, USG findings are not specific for this diagnosis.3,24
Computed tomography (CT) findings are more specific because a CT scan can show a fat component of the lesion clearly, which appears to be low in attenuation with Hounsfield units between −40 and −100.24,25 Although CT is more specific than USG, CT does have some disadvantages, including an inability to illustrate detailed uterine anatomy and confusion between an adnexal mass and a lesion arising from the uterus, particularly exophytic or pedunculated lesions3,24,26 as occurred in the current case.
MRI, with its multiplanar capabilities, is the most useful imaging modality for such differentiation, because MRI can reveal the uterine origin of the neoplasm.24,26 On MRI, the fatty component is high in signal intensity on both T1- and T2-weighted images. The fatty component of the lesion can also be confirmed by a fat-suppression sequence, which shows a decrease in signal intensity in fat components of the lesion. 25 Septa inside the mass can be seen on T1-weighted images. 25
The radiologic differential diagnoses of lipomatous masses in the pelvis include benign cystic teratomas of the ovaries; malignant degeneration of cystic teratomas; nonteratomatous, lipomatous ovarian tumors; benign pelvic lipomas; liposarcomas; extra-adrenal myelolipomas; angiomyolipomas; retroperitoneal cystic hamartomas; and lipoblastic lymphadenopathy.6,27,28
The various imaging features of a tumor in different modalities are important for determining the final diagnosis. Knowledge of these features is also important to radiologists, because most of these tumors are incidental findings on imaging. MRI is the modality of choice for the final diagnosis. 3 Asymptomatic lipoleiomyomas do not require any treatment.
Conclusions
The condition of the current patient together with a review of previous case reports reveals that, when a palpable mass is detected during a manual gynecologic examination in a postmenopausal or premenopausal patient, a gynecologist should consider the possibility of a lipoleiomyoma. Imaging is used to differentiate a lipoleiomyoma from an ovarian neoplasm because ovarian neoplasms are usually surgically excised, whereas lipoleiomyomas do not require any therapeutic intervention.
Footnotes
Disclosure Statement
No financial conflicts of interest exist.