
Abstract
Abstract
Introduction
M
Case
A 35-year-old multiparous woman was referred to the Postgraduate Institute of Medical Sciences (PGIMS), in Rohtak, Haryana, India, with a history of severe dysmenorrhea. She had reached menarche at age 14. A significant history of spasmodic dysmenorrhea was present since her menarche; this problem was relieved with antispasmodic drugs. In the 3 months prior to her presentation at PGIMS, this patient could no longer obtain relief from the antispasmodic drugs. She had been married for the prior 14 years and had experienced two full-term, uneventful vaginal deliveries, with her last childbirth occurring 10 years prior. This patient was referred to PGIMS a with a sonography scan and a magnetic resonance imaging (MRI) report suggestive of uterus didelphys and an absent left kidney. The sonography scan revealed a nonvisualized left kidney and a normally situated right kidney; the uterus was double with a hypertrophied cervix and a cystic lesion at the anterior lip of the cervix. The MRI revealed two separate uterine horns with the left uterus having fluid with altered echogenicity. There was a large cystic lesion on the left side of the cervix. The Left kidney was absent (Fig. 1). This patient was moderately built and nourished with normal vital signs. An abdominal examination revealed a slight tenderness in her lower abdomen. A speculum examination revealed a cystic swelling in her vagina, but her cervix was not visualized. On vaginal examination, only one cervix was felt posteriorly at the 6 o'clock position and a cystic mass was felt in the left lateral vaginal wall. The exact size of the doubled uterus could not be discerned. The patient was admitted to the hospital, and an examination under anesthesia was performed. This examination revealed the presence of a single cervix on the right side and a uterus was also felt on the right side. A cystic 7×8–cm swelling was noted on the left side of the cervix and a firm globular structure was felt above the swelling, although it was not clear whether the mass was from the cervix or the uterus. Initially laparoscopy was planned, but this did not make it possible to differentiate a rudimentary horn from the doubled uterus, as the cervix was not visualized because of the cystic mass. Thus, the patient was then given a laparotomy, which revealed two uterine horns, with the left horn slightly more enlarged than right the right horn, with a swelling below the two uteri (Fig. 2). The right cervix was felt normally, but the left cervix was not palpable. A decision for a left hemihysterectomy was made, because the left uterus was thought to be a rudimentary horn as the left cervix was not felt. An incision over the cystic swelling exposed altered, dark-colored blood, and the left cervix was well-visualized within this cystic swelling (Fig. 3). The hemihysterectomy was completed. A vaginal examination revealed that the swelling had collapsed, Allis forceps were applied, and septal resection was performed. A diagnosis of uterus didelphys with obstucted hemivagina and ipsilateral renal agenesis was hence made.

Magnetic resonance image showing two separate uterine horns with the left uterus having fluid and a large cystic lesion on the left side of cervix.
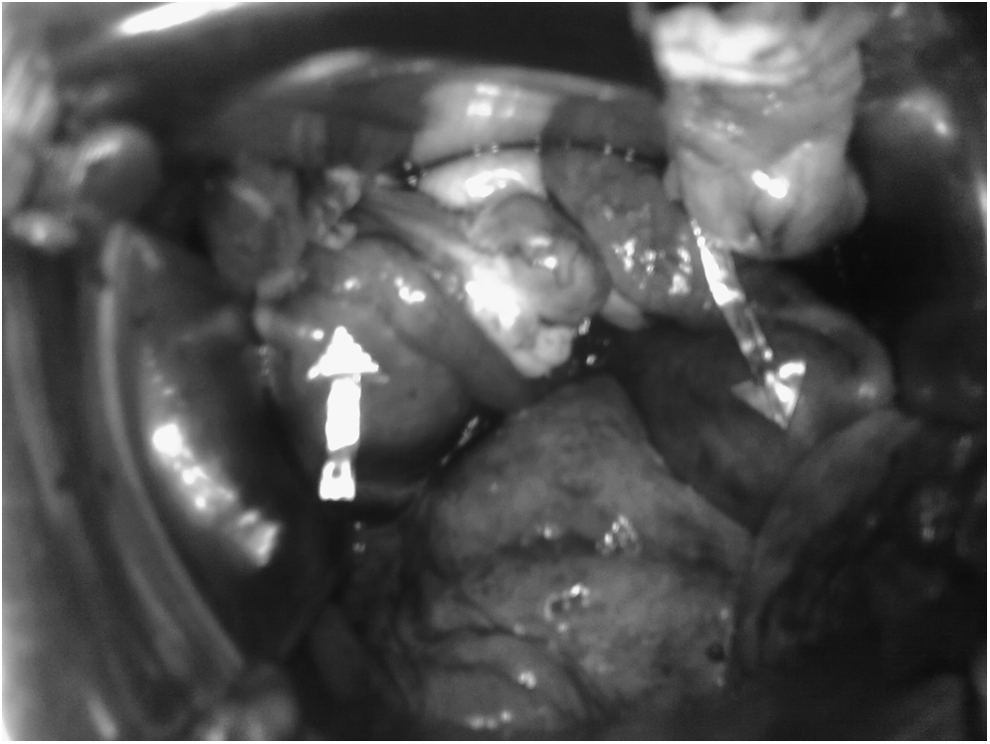
Laparotomy revealing two uterine horns (arrows).
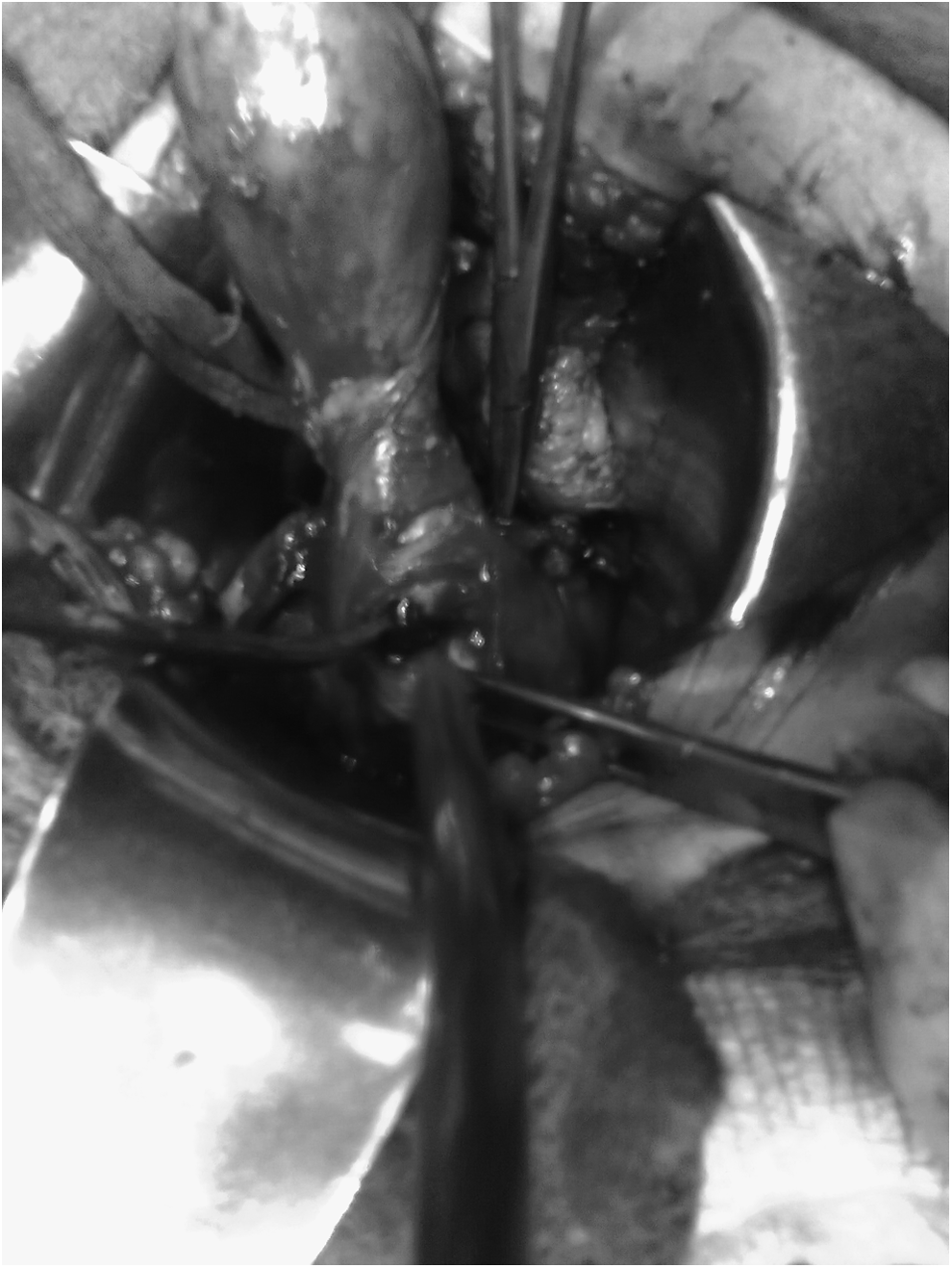
The left cervix well-visualized within the cystic swelling.
Results
The patient's postoperative period was uneventful and she was discharged after 5 days in the hospital.
Discussion
Anomalies of the internal female reproductive tract, referred to as Müllerian-duct anomalies, account for 7% of the female population. 2 In uterus didelphys, individual horns are fully developed and normal in size with two cervices being inevitably present. Each horn has one Fallopian tube and one ovary. A longitudinal or transverse vaginal septum may be noted. Uterus didelphys and obstructed hemivagina result from a genetic mutation at ∼4 weeks of gestation, which causes unilateral developmental abnormalities of the mesonephric ducts (Wolffian ducts), which displace the Müllerian ducts (paramesonephric ducts) laterally and prevent their fusion in the midline as well as with the urogenital sinus. Without a mesonephric duct, the ipsilateral ureter and kidney cannot develop, consequently HWW syndrome develops. 3 This was described in 1971 as Herlyn-Werner Syndrome, associated with renal agenesis and ipsilateral blind hemivagina. 4 The association of unilateral renal aplasia and bicornuate uterus with an isolated hematocervix and simple vagina was described in 1976 by Wunderlich. 5
Although the incidence of HWW syndrome is not known, that of uterus didelphys is 1/2000–1/28,000, accompanied by unilateral renal agenesis in 43% cases. 2 There are numerous reports of this syndrome presenting mostly soon after menarche. A review of the literature revealed reporting in as early as in a newborn to as late as in a young pregnant girl.7,8 Up to now, no case had been found to be reported in a middle-age multiparous woman. Table 1 lists case reports described in the literature. Diagnosis is usually made after menarche, but HWW syndrome's rarity and varied clinical presentation may contribute to diagnostic delays for years after menarche. These patients usually menstruate normally. The syndrome is suspected if there is progressively increasing dysmenorrhea or pelvic pain along with a vaginal or pelvic mass noted during a physical examination. The pelvic mass consists of a collection of blood products within the obstructed hemivagina and may extend upward to form an abdominal mass. The obstructing vaginal septum is usually oblique/longitudinal and varies in thickness from very thin to quite thick. Unusual presentations such as recurrent pyocolpos, urgency, frequency, chronic vaginal discharge, and ischiorectal swelling have also been reported.6,9
Because of its low cost, sonography is the easiest and first investigation. But MRI is the preferred modality for evaluating Müllerian-duct anomalies because of MRI's multiplanar capability and tissue characterization. Distance from a plane to the obstructed vagina can be calculated easily, which can be helpful for planning the surgery. 10 MRI also has been more sensitive for detecting the uterine contour, the shape of the intrauterine cavity, and the character of the septum, as well as revealing such associated aspects as endometriosis, pelvic inflammation, and adhesions. Laparoscopy is now considered to be more popular for evaluating female reproductive tract anomalies, although this procedure could be reserved for cases for which the diagnosis is not clear after imaging or when MRI is not available and not performed as a routine procedure. 11
The goals of treatment are to relieve the obstruction and perform remodeling of the vagina. The complications of chronic obstruction can be hematometra, pyometra, hematosalpinx, pyosalpinx, endometriosis, pelvic adhesions, and even infertility. Treatment for cases of Müllerian anomalies is individualized depending upon the age, complaints, and reproductive needs of each patient. Good knowledge of normal embryology and sexual differentiation is important for timely diagnosis and appropriate management. Resection of the vaginal septum and evacuation of retained old blood and mucus is a common method used especially in young adolescent females. In fewer cases, especially in women in their twenties, hemihysterectomy and excision of the vaginal septum has also been reported. The diagnosis in the current case was delayed owing to the distensibility of this patient's vagina and her use of nonsteroidal anti-inflammatory drugs, antispasmodic drugs, and oral contraceptive pills, which decreased the volume of her menstrual bleeding. Other reasons for diagnostic delay are resorption of blood in between a patient's periods and a poor understanding of Müllerian anomalies by both radiologists and gynecologists. In the current case, MRI—the “gold standard” test for diagnosis—was not very helpful, and a hematocolpos was mistaken as being a cystic lesion. Laparoscopy was not helpful for differentiating a rudimentary horn from a double uterus, as this patient's cervix was not visualized because of the collection of blood products. A hemihysterectomy was planned for the left uterine horn, because it was thought to be a rudimentary horn. During the hemihysterectomy it became clear that the cystic swelling was actually the obstructed hemivagina. The cervix was finally visualized later, confirming the diagnosis of a doubled uterus. Thus, another surgical team performed a septal resection from below the hematocolpos to drain it completely. Recurrent pyocolpos is a known complication in the cases of obstructed hemivagina, owing to the incomplete drainage caused by restenosis of the septectomy site. There was no issue regarding future pregnancies in this patient, as her family was complete; hence hemihysterectomy and septectomy were justified treatments for this patient.
Conclusions
Treatment should be individualized depending upon the class of Müllerian anomalies a patient has, along with her age, parity, and complaints.
Footnotes
Disclosure Statement
No competing financial conflicts exist.